Canine Valvular Heart Disease Study Guide
Canine Valvular Heart Disease
NAVLE Study Guide
Cardiovascular System | Species: Canine
Estimated Read Time: 35-40 minutes | Last Updated: December 2024
Overview and Clinical Importance
Valvular heart disease represents the most common category of acquired cardiovascular disease in dogs, accounting for approximately 75% of all canine heart disease cases. The most prevalent form is myxomatous mitral valve disease (MMVD), also known as degenerative valve disease, endocardiosis, or chronic valvular heart disease. Understanding the pathophysiology, diagnosis, staging, and treatment is essential for NAVLE success.
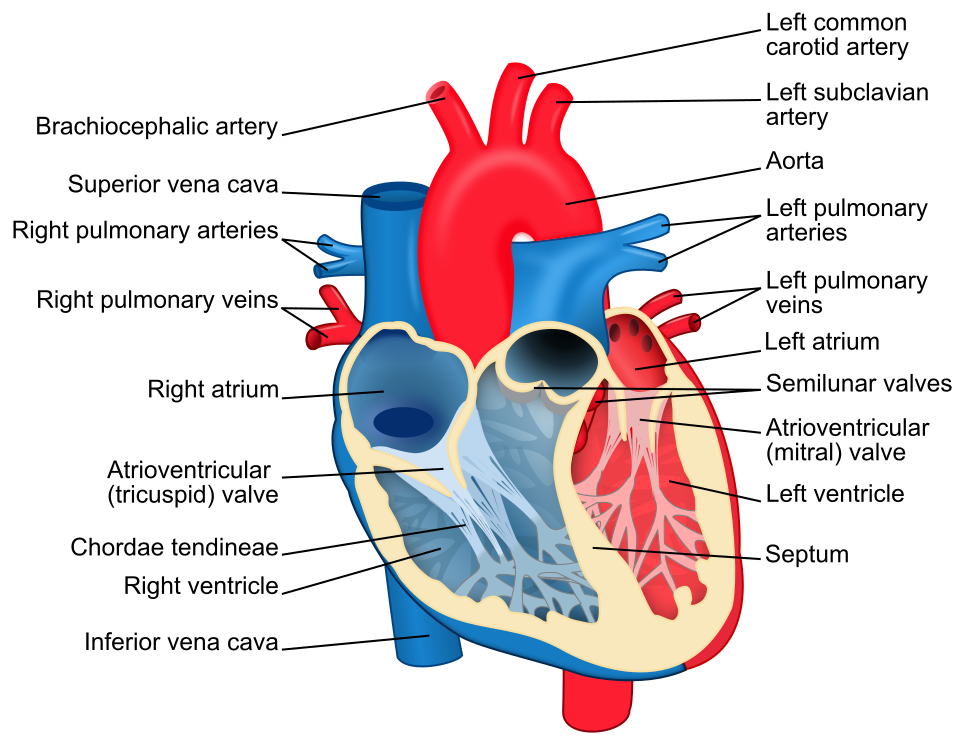
Figure 1 - Canine heart anatomy diagram showing all four cardiac valves - mitral, tricuspid, aortic, and pulmonic - with labeled chambers.
Learning Objectives
- Describe the pathophysiology and histopathologic changes in myxomatous mitral valve disease
- Apply the ACVIM staging system (A, B1, B2, C, D) to classify dogs with MMVD
- Interpret radiographic (VHS, VLAS) and echocardiographic (LA:Ao, LVIDdN) parameters
- Recognize breed predispositions for specific valvular diseases
- Formulate appropriate treatment plans based on disease stage
Myxomatous Mitral Valve Disease (MMVD)
Epidemiology and Breed Predisposition
MMVD is predominantly a disease of small to medium-sized dogs, with prevalence increasing markedly with age. Up to 85% of dogs in predisposed breeds show evidence of valve lesions by 13 years of age. The disease affects the mitral valve alone in approximately 60% of cases, both mitral and tricuspid in 30%, and tricuspid alone in less than 10%.
| High-Risk Breeds | Clinical Notes |
|---|---|
| Cavalier King Charles Spaniel | Highest prevalence; inherited trait; early onset; breeding restrictions recommended |
| Dachshund | Inherited trait; mitral valve prolapse common |
| Miniature/Toy Poodle, Chihuahua, Maltese | High prevalence in all small breeds; age-related |
High-Yield Note: On the NAVLE, when you see a geriatric small-breed dog with a left apical systolic murmur, MMVD should be at the top of your differential list. The Cavalier King Charles Spaniel is the classic breed association.
Pathophysiology
The pathophysiology involves progressive myxomatous degeneration characterized by: expansion of extracellular matrix with glycosaminoglycans; valvular interstitial cell transformation to myofibroblast phenotype; attenuation of the collagen-laden fibrosa layer; and chordae tendineae changes with potential rupture.
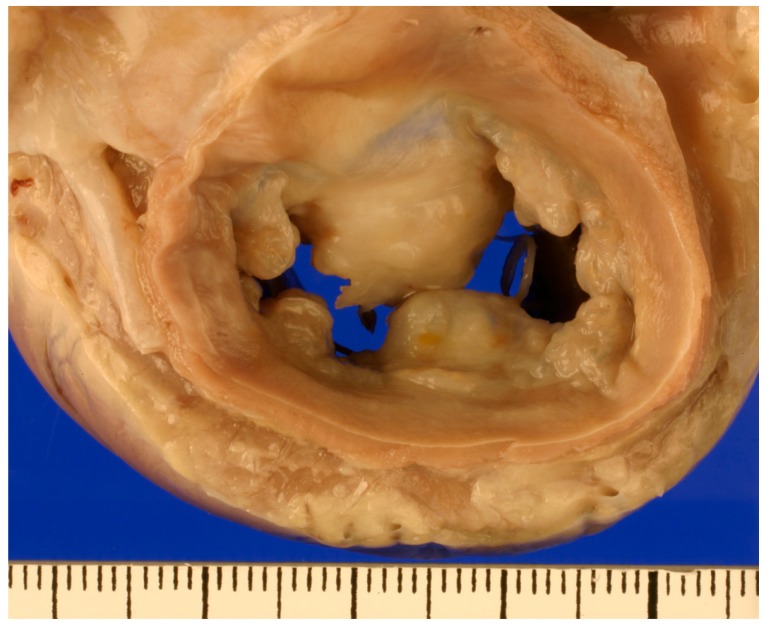
Figure 2 - Gross pathology of myxomatous mitral valve showing thickened, nodular valve leaflets
Reference: Menciotti G, Borgarelli M. Review of Diagnostic and Therapeutic Approach to Canine Myxomatous Mitral Valve Disease. Vet Sci. 2017 Sep 26;4(4):47. doi: 10.3390/vetsci4040047. PMID: 29056705; PMCID: PMC5753627.
Hemodynamic Cascade
- Systolic regurgitation from LV into LA creates volume overload
- Compensatory LA and LV dilation (eccentric hypertrophy)
- Increased LA pressure transmitted to pulmonary veins
- Pulmonary venous congestion and pulmonary edema (left-sided CHF)
- Secondary pulmonary hypertension may develop
Memory Tip: "LEAKY VALVE = VOLUME OVERLOAD" - MR causes volume (not pressure) overload, leading to eccentric (not concentric) hypertrophy.
Clinical Presentation
- Murmur: Left apical systolic (holosystolic); intensity correlates with severity
- PMI: Left 5th-6th intercostal space
- CHF signs: Cough (nocturnal), tachypnea, dyspnea, exercise intolerance, syncope
High-Yield Note: Sleeping respiratory rate (SRR) monitoring is critical. Normal SRR is less than 30 breaths/min. SRR greater than 40 suggests CHF.
ACVIM Staging System for MMVD
The ACVIM consensus staging system (2019 update) guides diagnosis and treatment. This is essential knowledge for the NAVLE.
| Stage | Description | Treatment |
|---|---|---|
| A | At-risk breeds; no murmur | No treatment; annual screening |
| B1 | Murmur present; no cardiac remodeling; LA:Ao less than 1.6 and/or LVIDdN less than 1.7 | No medication; monitor 6-12 months |
| B2 | Asymptomatic with remodeling. ALL 4 criteria: Murmur ≥3/6, LA:Ao ≥1.6, LVIDdN ≥1.7, VHS greater than 10.5 | Pimobendan 0.25-0.3 mg/kg PO q12h; dietary modification |
| C | Current/past CHF signs; pulmonary edema | Triple therapy: Furosemide + Pimobendan + ACE-I; add spironolactone |
| D | Refractory CHF; furosemide greater than 8 mg/kg/day | Increase diuretics; add torsemide/HCTZ; amlodipine; consider surgery |
Memory Tip - B2 Criteria: "ALL FOUR to treat before CHF" - Murmur ≥3/6, LA:Ao ≥1.6, LVIDdN ≥1.7, VHS greater than 10.5. Missing one = Stage B1 = no treatment.
Board Tip: The EPIC study showed pimobendan at Stage B2 delays CHF onset by ~15 months and reduces cardiac death risk by one-third. This landmark study is frequently referenced!
Diagnostic Evaluation
Key Parameters
| Parameter | B2 Criterion | Notes |
|---|---|---|
| VHS | Greater than 10.5 | Greater than 11.5 = significant cardiomegaly (can substitute for echo) |
| VLAS | ≥2.5 suggests LA enlargement | Useful when echo unavailable; 87% specific for LA:Ao ≥1.6 |
| LA:Ao Ratio | ≥1.6 | Right parasternal short-axis at AV level; early diastole |
| LVIDdN | ≥1.7 | Formula: LVIDd (cm) / BW (kg)^0.294 |
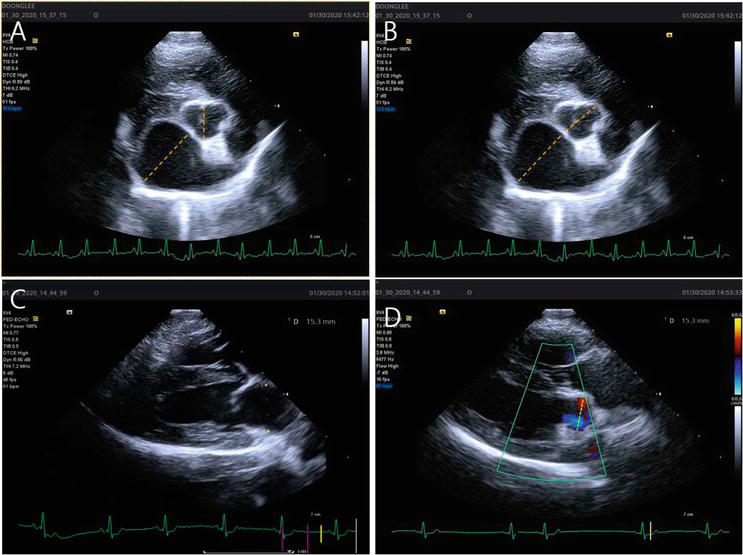
Figure 3 - Echocardiographic LA:Ao measurement in right parasternal short-axis view. The method for measurement of left atrial to aortic root ratio (LA/Ao). (A) A LA/Ao obtained from a right parasternal short axis (LA/AoSx) by method 1 (see text). (B) A LA/Ao obtained from a right parasternal short axis (LA/AoSx) by method 2 (see text). (C and D) A LA/Ao obtained from a right parasternal long axis (LA/AoLx). For LA diameter (C), the measurement was made at end-systole 1 to 2 frames before the opening of the mitral valve leaflets. The measurement bisects the atrium extending from the mid-atrial septum in the near field to the bright pericardial echo of the LA lateral wall in the far field and is roughly parallel to the mitral annulus. For Ao diameter (D), the measurement of the aortic valve was made between the opened aortic valve leaflets in an early systolic frame when the Ao diameter is the greatest.
Reference: https://www.intechopen.com/chapters/71522 DOI: 10.5772/intechopen.91819
Treatment of MMVD
Pimobendan (Vetmedin)
An inodilator combining positive inotropic effects with vasodilation via calcium sensitization and PDE-III inhibition. Dose: 0.25-0.3 mg/kg PO every 12 hours. Give 1 hour before or 2 hours after food. Start at Stage B2 or C/D.
Stage C Triple Therapy
- Furosemide: Loop diuretic; 2-4 mg/kg PO BID-TID maintenance
- Pimobendan: 0.25-0.3 mg/kg PO q12h
- ACE inhibitor: Enalapril/benazepril 0.5 mg/kg PO q12-24h
- Spironolactone: 2 mg/kg PO q12-24h (quadruple therapy)
High-Yield Note: Do NOT start beta-blockers in dogs actively showing CHF signs - this is a common exam pitfall!
Prognosis
- Stage B1: Excellent; many never progress
- Stage B2 with pimobendan: ~3.5 years to CHF
- Stage C: Median 9-15 months survival
- Stage D: 3-6 months survival
Congenital Valvular Diseases
Tricuspid Valve Dysplasia (TVD)
Congenital malformation causing tricuspid regurgitation and right heart volume overload. Labrador Retrievers have highest predisposition (heritable - chromosome 9). Presents with ascites, jugular distension, right-sided murmur. Treatment: medical management of right-sided CHF.
High-Yield Note: Young Labrador with ascites and right-sided systolic murmur = think TVD. Affected dogs should not be bred.
Pulmonic Stenosis (PS)
Third most common congenital defect. Breeds: English/French Bulldogs, Boston Terriers, Samoyeds, Labs. Type A (dome-shaped, fused leaflets) vs Type B (hypoplastic annulus in brachycephalics). Severity by gradient: less than 50 mmHg (mild), 50-80 mmHg (moderate), greater than 80 mmHg (severe - balloon valvuloplasty indicated).
Memory Tip: "50-80-Risk" - Less than 50 mmHg = mild; 50-80 mmHg = moderate; Greater than 80 mmHg = severe (intervene!).
Infective Endocarditis
Bacterial infection of heart valves (usually aortic/mitral). Predisposing factors: subaortic stenosis (most important), immunosuppression, chronic infections. Common organisms: Staph, Strep, E. coli, Bartonella. Clinical signs: fever, shifting leg lameness, new murmur, weight loss. Echocardiography shows vegetations. Treatment: prolonged IV antibiotics (6-8 weeks).
Board Tip: Antimicrobial prophylaxis IS indicated for dogs with SAS undergoing procedures. It is NOT indicated for dogs with MMVD - they are not at increased IE risk!
Practice Question
| A 10-year-old MN Cavalier King Charles Spaniel presents for wellness. The owner reports the dog is active with no cough or respiratory changes. Physical exam reveals a Grade 4/6 left apical systolic murmur. Radiographs show VHS of 11.2. Echocardiography reveals thickened, prolapsing mitral valve leaflets with LA:Ao ratio of 1.8 and LVIDdN of 1.85. What is the most appropriate next step? A. No treatment; recheck in 6-12 months B. Start furosemide 2 mg/kg PO BID C. Start pimobendan 0.25 mg/kg PO q12h D. Start enalapril 0.5 mg/kg PO BID E. Start triple therapy (furosemide + pimobendan + enalapril) |
|---|
Correct Answer: C
Explanation
Starting pimobendan (C) is correct because this dog meets ALL FOUR ACVIM Stage B2 criteria: murmur ≥3/6 (has 4/6), LA:Ao ≥1.6 (has 1.8), LVIDdN ≥1.7 (has 1.85), VHS greater than 10.5 (has 11.2). The EPIC study showed pimobendan delays CHF by ~15 months.
A is incorrect - this would be Stage B1 management; this dog has remodeling.
B is incorrect - furosemide is for Stage C with CHF; this dog is asymptomatic.
D is incorrect - ACE inhibitors alone lack proven benefit in Stage B2.
E is incorrect - triple therapy is for Stage C; this dog has no CHF signs.
High-Yield Note: Stage B2 requires ALL FOUR criteria. If even one is missing, it's Stage B1 with no treatment indicated. CKCS is the classic breed for NAVLE MMVD questions.
Summary and Key Takeaways
- MMVD is the most common acquired heart disease in dogs - primarily small breeds, especially CKCS
- Myxomatous degeneration causes valve thickening, prolapse, and MR leading to volume overload
- ACVIM staging (A, B1, B2, C, D) guides treatment; Stage B2 = ALL 4 criteria for pimobendan
- Echocardiography gold standard; key values: LA:Ao ≥1.6, LVIDdN ≥1.7
- Stage C = Triple therapy: furosemide + pimobendan + ACE-I
- TVD - Labradors; right-sided CHF with ascites
- PS severity by gradient; greater than 80 mmHg = balloon valvuloplasty
- IE - fever, shifting lameness, new murmur; prolonged antibiotics
Image Sources
- Wikimedia Commons - Heart Diagram with Valve Labels (CC BY-SA 3.0). URL: https://commons.wikimedia.org/wiki/File:Heart_diagram-en.svg
- PMC Open Access - Gross Pathology of MMVD. Borgarelli M et al. Animals. 2017;7(12):95. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC5753627/
- IntechOpen (CC BY 3.0) - Canine Echo LA:Ao. Kim HT, Han JI. URL: https://www.intechopen.com/chapters/71522
References
- Keene BW, Atkins CE, Bonagura JD, et al. ACVIM consensus guidelines for MMVD in dogs. J Vet Intern Med. 2019;33(3):1127-1140.
- Boswood A, Häggström J, Gordon SG, et al. EPIC Study—Pimobendan in Preclinical MMVD. J Vet Intern Med. 2016;30(6):1765-1779.
- Borgarelli M, et al. Review of Canine MMVD. Animals. 2017;7(12):95.
- Merck Veterinary Manual. Myxomatous AV Valve Degeneration. 2024.
- Merck Veterinary Manual. Infectious Endocarditis in Dogs and Cats. 2024.
- Cornell University CVM. Pulmonic Stenosis in Dogs. URL: https://www.vet.cornell.edu/
Practice NAVLE Questions
Test your knowledge with 10,000+ exam-style questions, detailed explanations, and timed exams.
Start Your Free Trial →