Canine Congestive Heart Failure Study Guide
Canine Congestive Heart Failure Study Guide
NAVLE Examination Preparation
Cardiovascular System | Species: Canine
Estimated Read Time: 35-45 minutes | Last Updated: December 2024
Overview and Clinical Importance
Congestive heart failure (CHF) is a clinical syndrome that occurs when the heart can no longer pump sufficient blood to meet the body's metabolic demands, or can only do so at elevated filling pressures. In dogs, CHF most commonly results from myxomatous mitral valve disease (MMVD), accounting for approximately 75% of all canine heart disease cases. The second most common cause is dilated cardiomyopathy (DCM), which predominantly affects large and giant breed dogs. Understanding the pathophysiology, clinical presentation, diagnostic approach, and treatment of CHF is essential for NAVLE success and clinical practice.
Heart failure in dogs carries significant morbidity and mortality. Approximately 10% of dogs presented to primary care veterinary practices have heart disease, making cardiovascular conditions a major component of the NAVLE examination. Early recognition and appropriate staging of heart disease directly impacts treatment decisions and patient outcomes.
Learning Objectives
- Classify congestive heart failure using the ACVIM staging system (Stages A through D)
- Differentiate between left-sided and right-sided heart failure based on clinical signs
- Identify breed predispositions for MMVD and DCM
- Interpret radiographic and echocardiographic findings consistent with CHF
- Select appropriate pharmacologic therapy for acute and chronic CHF management
- Understand the clinical significance of the EPIC trial for preclinical disease management
Pathophysiology of Congestive Heart Failure
Hemodynamic Basis
Heart failure develops when cardiac output becomes insufficient to meet tissue oxygen demands. The failing heart triggers compensatory mechanisms including:
- Renin-Angiotensin-Aldosterone System (RAAS) activation: Causes sodium and water retention, vasoconstriction, and cardiac remodeling
- Sympathetic nervous system activation: Increases heart rate and contractility but also increases myocardial oxygen demand
- Cardiac remodeling: Chamber dilation and hypertrophy that initially maintains output but eventually becomes maladaptive
- Natriuretic peptide release: Counterregulatory mechanism attempting to promote natriuresis and vasodilation
High-Yield Note: When left atrial pressure exceeds 25 mmHg, pulmonary edema develops. This is the hallmark of left-sided CHF and explains why dogs present with coughing and respiratory distress.
Left-Sided vs. Right-Sided Heart Failure
Understanding the anatomic basis of CHF helps predict clinical signs and guides diagnostic interpretation.
| Left-Sided CHF | Right-Sided CHF |
|---|---|
| Pathophysiology: Blood backs up into pulmonary veins Elevated left atrial pressure Fluid leaks into pulmonary interstitium and alveoli |
Pathophysiology: Blood backs up into systemic veins Elevated right atrial pressure Fluid accumulates in body cavities |
| Clinical Signs: Cough (especially at night) Tachypnea, dyspnea Orthopnea Pulmonary crackles Exercise intolerance Syncope |
Clinical Signs: Ascites (abdominal distension) Jugular venous distension Hepatomegaly Peripheral edema Pleural effusion Weight gain |
| Common Causes: MMVD (most common) DCM Patent ductus arteriosus Aortic stenosis |
Common Causes: Tricuspid valve disease Heartworm disease Pulmonic stenosis DCM (biventricular) |
Board Tip: Left-sided CHF is far more common in dogs than right-sided CHF. When you see a small breed dog with a heart murmur, cough, and tachypnea, think MMVD with left-sided CHF first. When you see ascites and jugular distension, think right-sided or biventricular failure.
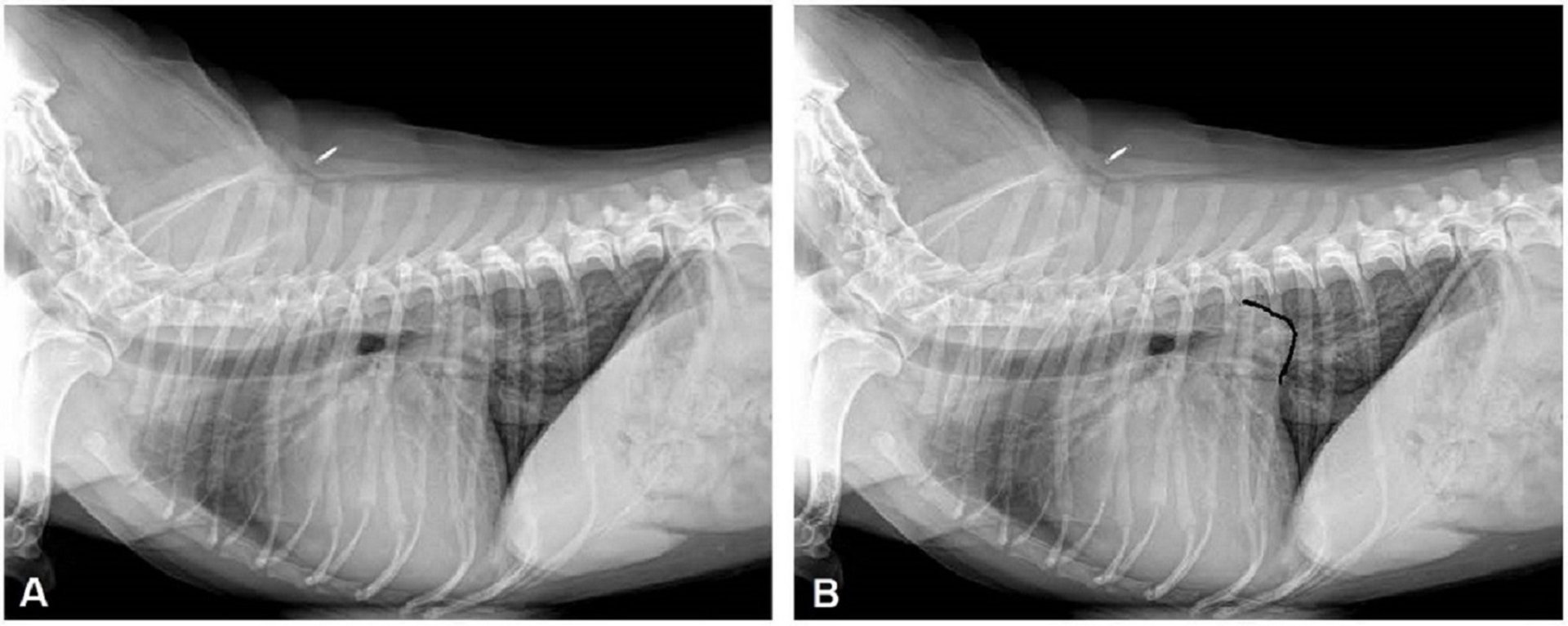
Figure 1 - Lateral thoracic radiograph of a dog with left-sided CHF showing cardiomegaly with left atrial enlargement, dorsal elevation of the trachea, and perihilar pulmonary edema pattern. (A). cardiogenic pulmonary edema due to severe mitral regurgitation and (B) body of the left atrium almost touching the spine. Courtesy of Dr. Mark D. Kittleson. Accessed from https://www.merckvetmanual.com/multimedia/image/congestive-heart-failure-dog-radiograph
ACVIM Staging System for Heart Disease
The American College of Veterinary Internal Medicine (ACVIM) consensus guidelines provide a standardized staging system that guides treatment decisions. This staging system is adapted from human medicine and is essential knowledge for the NAVLE.
| Stage | Definition | Management |
|---|---|---|
| A | High risk for developing heart disease No structural changes Examples: CKCS, Dobermans, Boxers |
No treatment indicated Regular screening recommended Client education |
| B1 | Structural heart disease present (murmur) No cardiac remodeling/enlargement Asymptomatic |
No treatment indicated Monitor every 6-12 months Radiographs and echocardiography as needed |
| B2 | Structural heart disease with cardiac remodeling Evidence of cardiomegaly (LA/Ao greater than or equal to 1.6, LVIDdN greater than or equal to 1.7) Asymptomatic |
Pimobendan indicated (EPIC study) Monitor every 4-6 months Home respiratory rate monitoring |
| C | Current or past clinical signs of CHF Responds to standard therapy Pulmonary edema or effusions present |
Triple therapy: Furosemide + Pimobendan + ACE inhibitor Consider spironolactone Sodium restriction |
| D | End-stage/Refractory CHF Does not respond to standard therapy Requires escalating doses of diuretics |
Increase furosemide (up to 8-12 mg/kg/day) Add torsemide or hydrochlorothiazide Sildenafil for pulmonary hypertension Quality of life assessment |
High-Yield Note: The EPIC study (2016) revolutionized treatment of preclinical heart disease. Dogs with Stage B2 MMVD treated with pimobendan had a median 15-month delay in onset of CHF compared to placebo. This is why pimobendan is now indicated for Stage B2 disease, not just Stage C.
Common Causes of Canine CHF
Myxomatous Mitral Valve Disease (MMVD)
MMVD is the most common acquired heart disease in dogs, accounting for approximately 75% of canine cardiovascular disease. It is characterized by progressive myxomatous degeneration of the mitral valve leaflets, causing mitral regurgitation.
Breed Predispositions
- Cavalier King Charles Spaniel: Highest prevalence, often develops at younger age (may have murmur by 1-2 years)
- Other small breeds: Miniature Poodle, Chihuahua, Miniature Schnauzer, Cocker Spaniel, Dachshund, Yorkshire Terrier
- Age: Prevalence increases with age; up to 85% of small breed dogs show evidence by 13 years
- Sex: Males affected 1.5 times more commonly than females
Clinical Findings
- Murmur: Left apical systolic murmur, grade increases with disease severity
- Radiography: Left atrial enlargement (dorsal deviation of trachea, splaying of mainstem bronchi), left ventricular enlargement, pulmonary venous distension
- Echocardiography: Thickened, prolapsing mitral valve leaflets; mitral regurgitation on color Doppler; LA/Ao ratio greater than or equal to 1.6 indicates significant enlargement
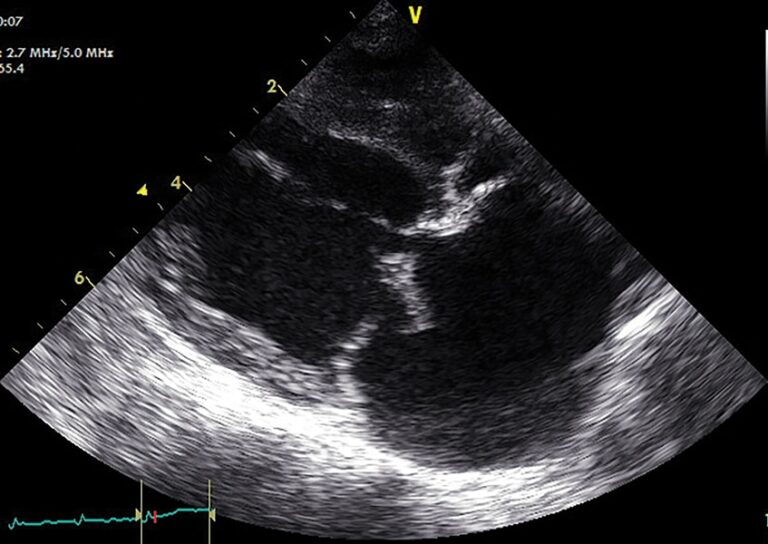
Figure 2 - Echocardiogram showing mitral valve regurgitation with color Doppler flow and left atrial enlargement in a dog with MMVD. Image credit: https://todaysveterinarypractice.com/cardiology/congestive-heart-failure-in-dogs/
Dilated Cardiomyopathy (DCM)
DCM is characterized by progressive loss of myocardial contractility with ventricular dilation and wall thinning. It predominantly affects large and giant breed dogs and carries a more guarded prognosis than MMVD.
Breed Predispositions
| Breed | Unique Features | Prognosis |
|---|---|---|
| Doberman Pinscher | High incidence of ventricular arrhythmias Sudden death common Genetic mutations (PDK4, TTN) Approximately 60% lifetime risk |
Poorest prognosis Median survival 3-6 months after CHF 3% survival at 1 year |
| Boxer | Arrhythmogenic right ventricular cardiomyopathy (ARVC) VPCs with LBBB morphology STRN gene mutation Syncope common |
Variable Sudden death risk high Sotalol often used |
| Great Dane | Often presents with atrial fibrillation Massive cardiomegaly |
Poor to guarded 6-24 months with treatment |
| Cocker Spaniel | May be taurine-responsive Slower progression |
Better than other breeds Check taurine levels |
Memory Tip - Doberman DCM: "Double Doom"
- Double screening: Echo AND Holter annually starting at age 3
- Double trouble: VPCs greater than 300/24hr OR 50-300 on two consecutive readings = diagnostic
- Double-digit survival: Only 3-6 months median survival after CHF develops
Diagnostic Approach
Physical Examination
- Auscultation: Murmur grade and location, arrhythmias, gallop sounds, pulmonary crackles
- Respiratory assessment: Rate, effort, orthopnea, cyanosis
- Pulse quality: Weak pulses suggest low output; pulse deficits indicate arrhythmia
- Jugular assessment: Distension or pulsations indicate right-sided failure
Thoracic Radiography
Radiography is the primary diagnostic tool for confirming CHF and is essential for staging.
| Measurement | Normal Value | Significance |
|---|---|---|
| Vertebral Heart Score (VHS) | 8.4-10.5 vertebrae (dogs) | Greater than 10.5 suggests cardiomegaly Greater than or equal to 11.5 = Stage B2 criterion |
| Vertebral Left Atrial Size (VLAS) | 1.8-2.3 vertebrae | Greater than 2.3 indicates LA enlargement More specific than VHS for LA size |
Radiographic Signs of Left-Sided CHF
- Cardiomegaly: Increased VHS, loss of waist, increased sternal contact
- Left atrial enlargement: Dorsal elevation of trachea and carina, splaying of mainstem bronchi
- Pulmonary venous distension: Veins larger than accompanying arteries
- Pulmonary edema: Perihilar to caudodorsal distribution, interstitial to alveolar pattern
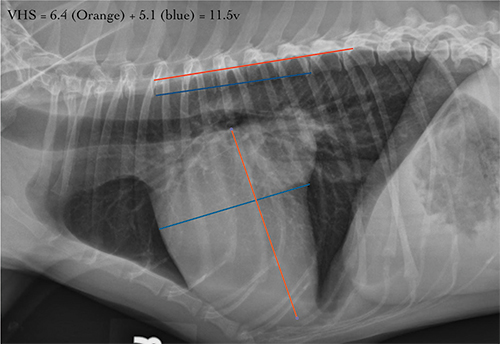
Figure 3 – VHS (moderate cardiomegaly in a dog with a VHS of 11.5) measurement technique on lateral thoracic radiograph demonstrating how to measure the long and short axis of the heart and compare to vertebral bodies starting at T4.
Reference and image credit: https://vetmed.illinois.edu/2022/07/06/evaluating-the-heart-size-on-radiographs/
Echocardiography
Echocardiography is the gold standard for diagnosing underlying cardiac disease and assessing severity.
| Parameter | Stage B2 Criterion | What It Indicates |
|---|---|---|
| LA/Ao Ratio | Greater than or equal to 1.6 | Left atrial dilation from volume overload |
| LVIDdN | Greater than or equal to 1.7 | Left ventricular dilation |
| Fractional Shortening | 25-45% (normal) | Low FS indicates systolic dysfunction (DCM) High FS in MMVD from volume overload |
Board Tip: In MMVD, fractional shortening is often ELEVATED (greater than 45%) due to volume overload, not decreased. A low or low-normal FS in advanced MMVD is a poor prognostic sign suggesting myocardial failure is developing.
Treatment of Congestive Heart Failure
Emergency Management of Acute CHF
Dogs presenting in acute respiratory distress require immediate stabilization. Minimize stress - even handling for diagnostics can be fatal in severely compromised patients.
Initial Stabilization Protocol
- Oxygen supplementation: Flow-by, oxygen cage, or nasal cannula
- Furosemide IV bolus: 2-4 mg/kg IV or IM; repeat every 30-60 minutes until respiratory rate decreases
- Furosemide CRI (alternative): 0.66-1 mg/kg/hour IV
- Pimobendan: 0.25-0.3 mg/kg PO; onset of action within 1 hour
- Sedation if needed: Butorphanol 0.2-0.4 mg/kg IV or IM for anxiety/dyspnea
High-Yield Note: NEVER give IV fluids to a patient in acute CHF - they already have volume overload! Allow free access to water once diuresis begins, but IV fluid administration is contraindicated.
Chronic Management - Drug Therapy
| Drug Class | Drug/Dose | Mechanism | Key Points |
|---|---|---|---|
| Loop Diuretic | Furosemide 1-2 mg/kg PO q12h (start) Up to 4-6 mg/kg q8h |
Inhibits Na/K/2Cl cotransporter in loop of Henle | Monitor renal values, electrolytes PU/PD expected Lowest effective dose |
| Inodilator | Pimobendan 0.25-0.3 mg/kg PO q12h Give on empty stomach |
Calcium sensitizer PDE III inhibitor Positive inotrope + vasodilator |
Start at Stage B2 (EPIC) Prolongs survival No monitoring needed |
| ACE Inhibitor | Enalapril 0.25-0.5 mg/kg PO q12-24h OR Benazepril 0.25-0.5 mg/kg PO q24h |
Inhibits ACE Reduces angiotensin II Decreases afterload |
Start at Stage C Monitor renal values Recheck 7-14 days after starting |
| Aldosterone Antagonist | Spironolactone 0.5-2 mg/kg PO q12-24h |
Aldosterone receptor antagonist Potassium-sparing Antifibrotic effects |
Prolongs survival (BESST trial) Weak diuretic alone Helps prevent hypokalemia |
Memory Tip - CHF Drug Therapy: "FAPS"
- F = Furosemide (loop diuretic)
- A = ACE inhibitor (enalapril/benazepril)
- P = Pimobendan (inodilator)
- S = Spironolactone (aldosterone antagonist)
Refractory Heart Failure (Stage D)
When standard therapy fails, escalation strategies include:
- Increase furosemide frequency: q8h or even q6h dosing
- Switch to torsemide: More potent loop diuretic with better bioavailability; dose at approximately 10% of furosemide dose
- Add hydrochlorothiazide: 0.5-1 mg/kg PO q24h for sequential nephron blockade
- Sildenafil: 1-2 mg/kg PO q8-12h for pulmonary hypertension
- Increase pimobendan: Off-label doses up to 0.4 mg/kg TID have been used safely
Prognosis and Survival
| Condition | Median Survival After CHF | Prognostic Factors |
|---|---|---|
| MMVD (Stage C) | 6-14 months (median approximately 9 months) | LA size, LV size Mitral E wave velocity Body weight loss |
| DCM (non-Doberman) | 6 months (most die within 6 months) | Severity of CHF at presentation Presence of arrhythmias Taurine-responsiveness |
| DCM (Doberman) | 3-6 months (poorest prognosis) | High sudden death risk VPC burden 3% survival at 1 year |
| Stage D (any cause) | Approximately 281 days (range highly variable) | Response to therapy escalation Renal function Cardiac cachexia |
High-Yield Note: Cardiac cachexia (unintended weight loss with muscle wasting) is a poor prognostic indicator. Dogs losing weight despite adequate caloric intake have activation of catabolic pathways and advanced disease.
Landmark Clinical Trials
EPIC Study (2016)
- Population: 360 dogs with Stage B2 MMVD
- Intervention: Pimobendan vs. placebo
- Result: Median 15-month delay in onset of CHF with pimobendan
- Clinical significance: Changed standard of care - pimobendan now indicated for Stage B2
QUEST Study
- Finding: Pimobendan superior to benazepril alone for Stage C MMVD
BESST Trial
- Finding: Adding spironolactone to ACE inhibitor improves outcomes
PROTECT Study
- Finding: Pimobendan delays CHF onset by approximately 9 months in preclinical Doberman DCM
Practice Question
| An 11-year-old male neutered Cavalier King Charles Spaniel presents with a 2-week history of progressive cough that worsens at night and mild exercise intolerance. The owner reports the dog has seemed more tired than usual. On physical examination, you auscultate a grade IV/VI left apical systolic heart murmur and fine crackles in the caudodorsal lung fields bilaterally. Respiratory rate is 48 breaths per minute with slightly increased effort. Heart rate is 140 bpm and regular. Mucous membranes are pink with a CRT of 2 seconds. Thoracic radiographs reveal a vertebral heart score of 12.5, dorsal elevation of the trachea, and an interstitial to alveolar pattern in the perihilar region. Which of the following is the most appropriate initial treatment plan for this patient? A. Enalapril alone and recheck in 2 weeks B. Furosemide, pimobendan, and enalapril C. Pimobendan alone since the dog is in Stage B2 D. Atenolol to control heart rate E. Digoxin for positive inotropic support |
|---|
Correct Answer: B
Explanation
Furosemide, pimobendan, and enalapril (Option B) is correct because this patient is in Stage C congestive heart failure. The clinical evidence for CHF includes: nocturnal cough, exercise intolerance, tachypnea at rest (48 bpm is elevated), pulmonary crackles on auscultation, radiographic evidence of cardiomegaly (VHS 12.5 is markedly elevated), and pulmonary edema (perihilar interstitial-alveolar pattern). This patient requires "triple therapy" with a diuretic (furosemide) to remove pulmonary edema, an inodilator (pimobendan) for positive inotropy and afterload reduction, and an ACE inhibitor (enalapril) for neurohormonal modulation and afterload reduction.
Option A (Enalapril alone) is incorrect because ACE inhibitors alone are insufficient for treating active CHF. This patient has pulmonary edema and requires diuretic therapy. ACE inhibitors are important but do not directly remove fluid.
Option C (Pimobendan alone) is incorrect because this patient is NOT in Stage B2 - they have progressed to Stage C with active CHF. While pimobendan monotherapy is appropriate for Stage B2 (based on the EPIC study), patients with clinical signs of CHF require diuretics and typically ACE inhibitors as well.
Option D (Atenolol) is incorrect and potentially dangerous. Beta-blockers have negative inotropic effects and should never be administered to patients with acute CHF. The patient's heart rate of 140 bpm is a compensatory response and the tachycardia is appropriate - suppressing it would decrease cardiac output.
Option E (Digoxin) is incorrect because digoxin is no longer a first-line agent for CHF. Pimobendan has largely replaced digoxin due to superior efficacy and safety profile. Digoxin may be considered for rate control in atrial fibrillation but is not indicated as primary therapy here.
Board Tip: When you see a CKCS with a murmur, nocturnal cough, and radiographic evidence of cardiomegaly with pulmonary infiltrates, think MMVD with left-sided CHF (Stage C). The treatment is "triple therapy" - Furosemide + Pimobendan + ACE inhibitor. Remember that CKCS are highly predisposed to MMVD and can develop disease at a younger age than other breeds.
Summary - Key Takeaways
- CHF occurs when the heart cannot maintain adequate output; most common causes are MMVD (75%) and DCM
- Left-sided CHF causes pulmonary edema (cough, dyspnea); right-sided CHF causes ascites and peripheral edema
- ACVIM staging guides treatment: Stage B2 = pimobendan; Stage C = triple therapy (furosemide + pimobendan + ACE inhibitor)
- EPIC study: Pimobendan delays CHF onset by 15 months in Stage B2 MMVD
- VHS greater than 10.5 suggests cardiomegaly; VHS greater than or equal to 11.5 with LA/Ao greater than or equal to 1.6 defines Stage B2
- Acute CHF: Oxygen, IV furosemide (2-4 mg/kg), pimobendan; NEVER give IV fluids
- Prognosis: MMVD Stage C median survival 6-14 months; Doberman DCM has poorest prognosis (3-6 months)
- Beta-blockers are contraindicated in acute CHF due to negative inotropic effects
Image Sources
- Figure 1: Lateral thoracic radiograph - Congestive heart failure with pulmonary edema. Source: Merck Veterinary Manual - Multimedia. Available at: https://www.merckvetmanual.com/multimedia/image/congestive-heart-failure-dog-radiograph (Free educational use)
- Figure 2: Color Doppler echocardiogram showing mitral regurgitation. Source: Today's Veterinary Practice - "Congestive Heart Failure in Dogs: Treatment and Management" - Figure 4. Available at: https://todaysveterinarypractice.com/cardiology/congestive-heart-failure-in-dogs/ (Open access educational content)
- Figure 3: VHS measurement technique. Source: University of Illinois College of Veterinary Medicine - "Evaluating the Heart Size on Radiographs" - Figure 1. Available at: https://vetmed.illinois.edu/2022/07/06/evaluating-the-heart-size-on-radiographs/ (Educational institution - free access)
References
- Keene BW, Atkins CE, Bonagura JD, et al. ACVIM consensus guidelines for the diagnosis and treatment of myxomatous mitral valve disease in dogs. J Vet Intern Med. 2019;33:1127-1140.
- Boswood A, Häggström J, Gordon SG, et al. Effect of pimobendan in dogs with preclinical myxomatous mitral valve disease and cardiomegaly: The EPIC study—a randomized clinical trial. J Vet Intern Med. 2016;30:1765-1779.
- Atkins C, Bonagura J, Ettinger S, et al. Guidelines for the diagnosis and treatment of canine chronic valvular heart disease. J Vet Intern Med. 2009;23:1142-1150.
- Häggström J, Boswood A, O'Grady M, et al. Longitudinal analysis of quality of life, clinical, radiographic, echocardiographic, and laboratory variables in dogs with preclinical myxomatous mitral valve disease receiving pimobendan or placebo: The EPIC study. J Vet Intern Med. 2017;31:1569-1582.
- O'Grady MR, Minors SL, O'Sullivan ML, Horne R. Effect of pimobendan on case fatality rate in Doberman Pinschers with congestive heart failure caused by dilated cardiomyopathy. J Vet Intern Med. 2008;22:897-904.
- Bernay F, Bland JM, Häggström J, et al. Efficacy of spironolactone on survival in dogs with naturally occurring mitral regurgitation caused by myxomatous mitral valve disease. J Vet Intern Med. 2010;24:331-341.
- Merck Veterinary Manual. Congestive Heart Failure in Dogs and Cats. Available at: https://www.merckvetmanual.com
- Cornell University College of Veterinary Medicine. Canine Dilated Cardiomyopathy (DCM). Available at: https://www.vet.cornell.edu/hospitals/services/cardiology/canine-dilated-cardiomyopathy-dcm
Practice NAVLE Questions
Test your knowledge with 10,000+ exam-style questions, detailed explanations, and timed exams.
Start Your Free Trial →