Canine Intussusception Study Guide
Canine Intussusception Study Guide
NAVLE Study Guide
Gastrointestinal and Digestive System | Species: Canine
Estimated Read Time: 30-35 minutes | Last Updated: December 2024
Overview and Clinical Importance
Intussusception is the invagination (or telescoping) of one segment of the gastrointestinal tract into the lumen of an adjacent segment. The invaginated segment is termed the intussusceptum, while the enveloping outer segment is called the intussuscipiens. This condition represents a surgical emergency in veterinary medicine because it leads to intestinal obstruction, compromised blood supply, tissue necrosis, and potentially life-threatening peritonitis if left untreated.
Intussusception is a common cause of bowel obstruction in small animals and is most frequently encountered in young dogs (less than 1 year of age). The condition requires rapid recognition and surgical intervention for optimal patient outcomes. Understanding the etiology, clinical presentation, diagnostic approach, and surgical management is essential for NAVLE success.
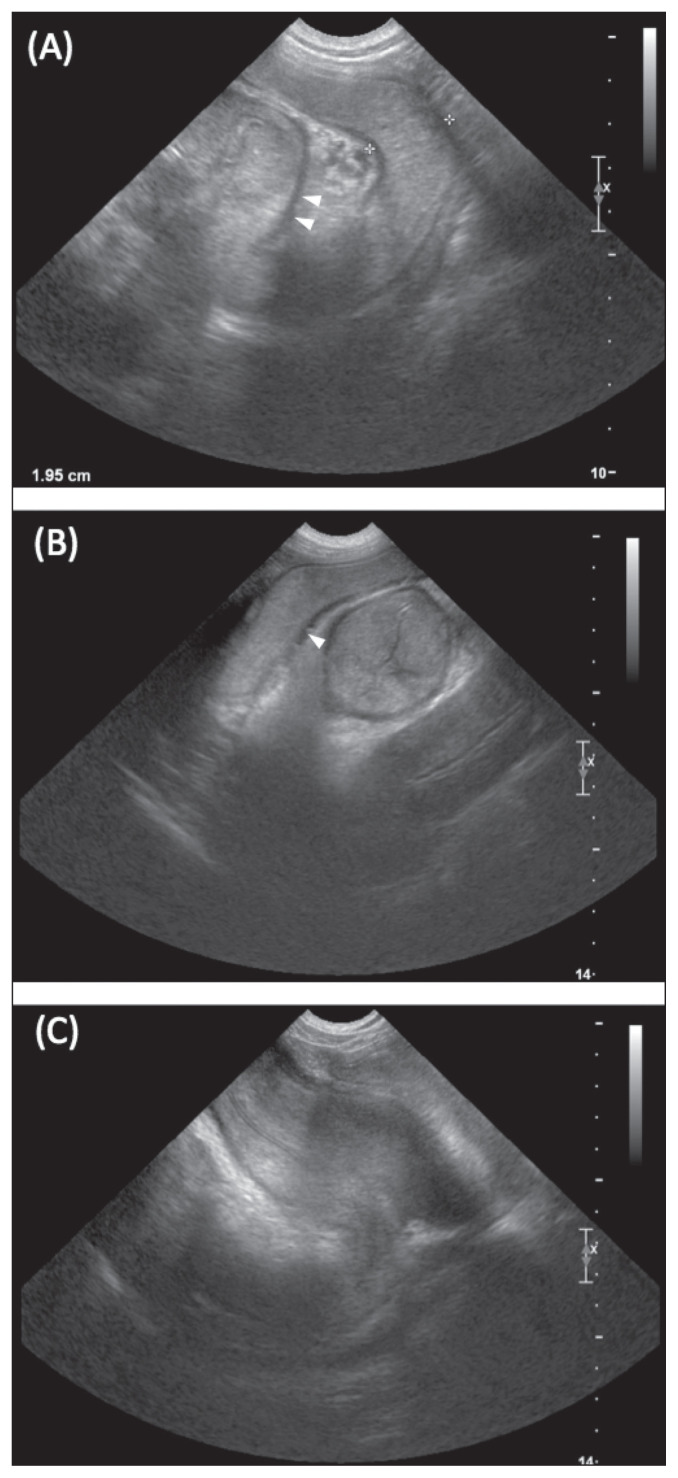
Figure 1. Diagram illustrating the anatomy of intussusception showing the intussusceptum (invaginated segment) telescoping into the intussuscipiens (enveloping segment), with the apex and neck clearly labeled.
Learning Objectives
- Define intussusception and understand the anatomical terminology (intussusceptum, intussuscipiens, apex, neck)
- Identify predisposing factors and underlying causes of intussusception in dogs
- Recognize clinical signs associated with acute and chronic intussusception
- Describe diagnostic imaging findings, particularly the pathognomonic ultrasound target sign
- Understand surgical treatment options including manual reduction, resection and anastomosis, and enteroplication
- Discuss prognosis, complications, and recurrence prevention strategies
Etiology and Pathophysiology
Mechanism of Intussusception
Intussusception occurs when there is abnormal intestinal motility characterized by a segment of hypermotile bowel adjacent to a segment with decreased motility (ileus). The hypermotile segment telescopes into the adjacent relaxed segment, typically in the direction of normal peristalsis (normograde or direct intussusception). Retrograde intussusception can occur but is less common.
The pathophysiology progresses as follows: initial invagination causes partial obstruction, which may progress to complete obstruction. The mesentery becomes trapped between the intussusceptum and intussuscipiens, leading to venous congestion and edema of the invaginated segment. Progressive constriction eventually compromises arterial blood flow, causing ischemia and necrosis. Fibrinous adhesions form between serosal surfaces, and if left untreated, bowel perforation and peritonitis develop.
Predisposing Factors and Underlying Causes
Any condition causing intestinal inflammation (enteritis) or altered motility can predispose to intussusception. In approximately 67% of cases, no identifiable cause is found (idiopathic). The most common predisposing factors include:
| Category | Specific Causes |
|---|---|
| Viral Enteritis | Canine parvovirus (most common infectious cause), Canine distemper virus, Coronavirus |
| Intestinal Parasites | Roundworms (Toxocara), Hookworms (Ancylostoma), Whipworms (Trichuris), Giardia |
| Bacterial Enteritis | Salmonella, Clostridium, Campylobacter |
| Foreign Bodies | Linear foreign bodies (string, yarn), Non-digestible objects (bones, toys) |
| Previous Surgery | Post-abdominal surgery, Post-enterotomy |
| Neoplasia (older dogs) | Intestinal lymphoma, Adenocarcinoma, Leiomyoma/Leiomyosarcoma |
| Other | Inflammatory bowel disease, Dietary indiscretion, Metabolic disorders |
High-Yield Note: Canine parvovirus is a major predisposing factor for intussusception. If a dog with parvoviral enteritis shows sudden clinical deterioration, persistent vomiting despite antiemetics, or a palpable abdominal mass, always consider intussusception as a complication!
Signalment and Breed Predispositions
Approximately 75% of dogs with intussusception are less than 1 year of age. Large breed dogs may be more commonly affected, although intussusception can occur in any breed. German Shepherds are particularly predisposed to gastroesophageal intussusception. When intussusception occurs in older dogs (greater than 3-4 years), neoplasia should be suspected as an underlying cause.
Types and Anatomical Locations
The most common location for intussusception in dogs is the ileocolic junction (ileum into colon/cecum), accounting for approximately 43-50% of cases. Jejunojejunal intussusception is the second most common type.
| Type | Location | Clinical Features |
|---|---|---|
| Ileocolic (Enterocolic) | Ileum into cecum/colon | Most common; tenesmus, hematochezia; may prolapse through rectum |
| Jejunojejunal (Enteroenteric) | Jejunum into jejunum | More severe obstructive pattern; more likely to cause complete obstruction |
| Gastroesophageal | Stomach into esophagus | Rare; German Shepherds predisposed; severe clinical signs; poor prognosis |
| Colocolic | Colon into colon | Less common; less severe clinical signs than small bowel involvement |
Board Tip: Remember "I-C-E" for the most common intussusception location: Ileum into Cecum/colon (Enterocolic). The severity of clinical signs generally increases the more proximal the obstruction - jejunojejunal intussusceptions typically cause more severe signs than ileocolic intussusceptions.
Clinical Signs and Presentation
Clinical signs vary based on the location of intussusception, degree of obstruction (partial vs. complete), duration, and presence of vascular compromise. Signs may be acute or chronic/intermittent.
Acute Presentation
- Vomiting - often persistent; may be bilious or contain blood
- Diarrhea - frequently bloody (hematochezia) or mucoid; "currant jelly" appearance
- Abdominal pain - may present as hunched posture, reluctance to move
- Depression and lethargy
- Anorexia
- Dehydration - tachycardia, prolonged CRT, pale mucous membranes
Chronic Presentation
- Intermittent, intractable diarrhea
- Weight loss and emaciation
- Hypoalbuminemia - intussusception is one of the two major causes of protein-losing enteropathy in dogs less than 12 months of age (along with parasites)
- Intermittent episodes of obstruction that spontaneously resolve
Physical Examination Findings
- Palpable abdominal mass - reported in approximately 53% of cases; firm, tubular, "sausage-shaped" structure
- Abdominal distension
- Tenesmus (especially with ileocolic intussusception)
- Rectal prolapse of intussuscepted segment - distinguish from true rectal prolapse by attempting to pass a probe alongside the prolapsed tissue (impossible with intussusception, possible with rectal prolapse)
- Signs of shock in severe cases: tachycardia, weak pulses, prolonged CRT, hypothermia
High-Yield Note: Clinical signs may be INTERMITTENT! The intussusception can spontaneously reduce and then reform. Do not be falsely reassured by temporary improvement - surgical intervention is still typically required to prevent recurrence.
Diagnosis
Laboratory Findings
Laboratory abnormalities are often nonspecific and reflect the underlying cause and degree of illness:
- CBC: Leukocytosis or leukopenia (if concurrent parvovirus), stress leukogram, hemoconcentration from dehydration
- Serum biochemistry: Electrolyte abnormalities (hypokalemia, hypochloremia), azotemia (prerenal), hypoalbuminemia in chronic cases, elevated lactate
- Fecal examination: To rule out parasites as underlying cause; parvovirus ELISA testing
Diagnostic Imaging
Abdominal Radiography
Plain radiographs have limited sensitivity (approximately 48%) for detecting intussusception. Findings may include:
- Signs of intestinal obstruction: dilated, gas/fluid-filled intestinal loops
- Soft tissue density mass effect in abdomen
- Decreased serosal detail (if peritonitis present)
- "Gravel sign" - granular appearance from trapped ingesta
Contrast (barium) studies may show a "coiled spring" appearance as contrast outlines the intussusception, but have largely been replaced by ultrasound.
Abdominal Ultrasonography - Gold Standard
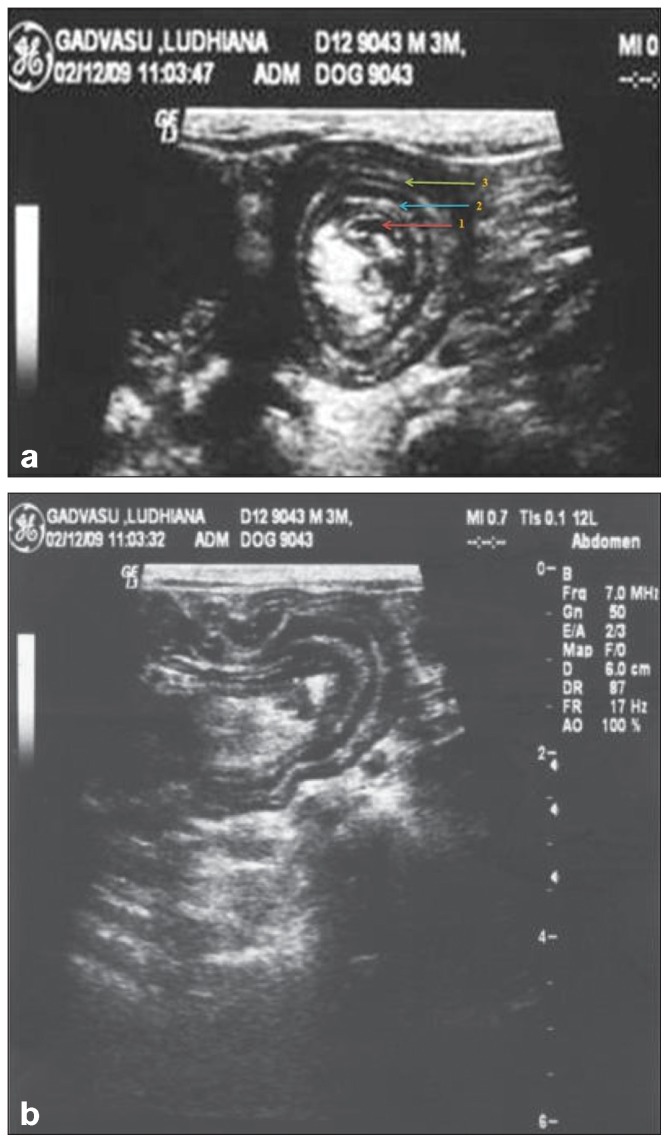
Figure 2. Transverse ultrasound view showing the pathognomonic target sign (also called bull's eye sign or doughnut sign) of intussusception, demonstrating concentric alternating hyperechoic and hypoechoic rings representing the layers of invaginated bowel.
| Ultrasound Finding | Description |
|---|---|
| Target Sign (Transverse) | Multiple (greater than 5) concentric alternating hyperechoic and hypoechoic rings; PATHOGNOMONIC for intussusception |
| Multiple Parallel Lines (Longitudinal) | Alternating hyperechoic and hypoechoic linear streaks; "sandwich sign" |
| Pseudokidney Sign | Seen when intussusception is curved and mesentery visible on one side; resembles kidney shape |
| Hyperechoic Crescent | Invaginated mesentery appears as hyperechoic semilunar structure; may see congested vessels within |
| Associated Findings | Proximal bowel dilation, fluid accumulation, hyperperistalsis (acute) or absence of peristalsis (chronic), peritoneal effusion |
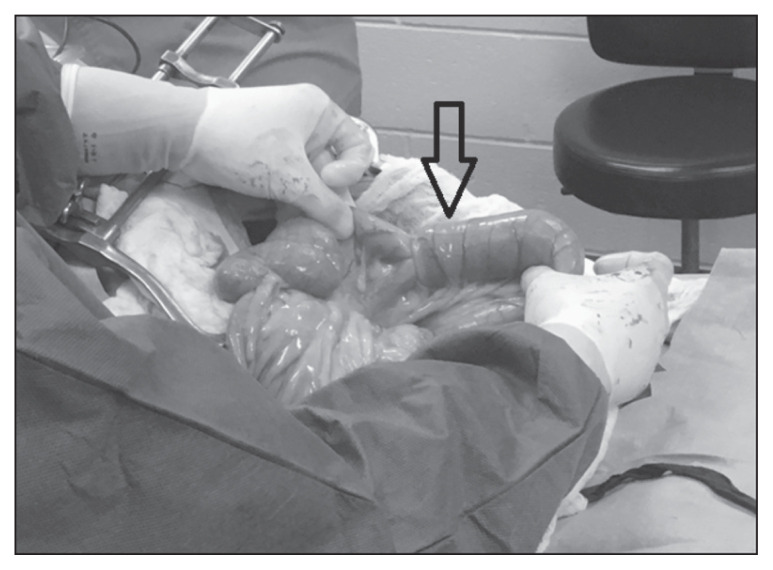
Figure 3. Longitudinal ultrasound view of intussusception showing multiple parallel hyperechoic and hypoechoic layers within the lumen of the intussuscipiens.
Board Tip - Memory Aid: "TARGET your diagnosis with ultrasound!" The TARGET SIGN is pathognomonic for intussusception. Think of it like looking at a dartboard (target) from above - you see concentric rings. On longitudinal view, you see "stacked pancakes" or parallel lines.
Doppler Ultrasound for Reducibility Prediction
Color Doppler assessment of blood flow to the intussusceptum can help predict reducibility and bowel viability. Absence of blood flow suggests non-viability and the need for resection rather than manual reduction.
Treatment
Preoperative Stabilization
Intussusception is a surgical emergency. However, patient stabilization prior to anesthesia is essential:
- IV fluid therapy: Correct dehydration and electrolyte imbalances (crystalloids; colloids if hypoalbuminemic)
- Broad-spectrum antibiotics: For bacterial translocation risk (ampicillin/sulbactam, or cefazolin plus metronidazole)
- Analgesia: Opioids (methadone, hydromorphone) - also help slow intestinal motility
- Address underlying cause: Continue parvovirus treatment if applicable
Surgical Options
| Procedure | Indications | Technique |
|---|---|---|
| Manual Reduction | Recent intussusception with viable bowel; minimal adhesions; reducible segment | Gentle milking of intussuscipiens away from intussusceptum (NEVER pull on intussusceptum); assess bowel viability post-reduction |
| Resection and Anastomosis | Non-reducible intussusception; non-viable bowel; adhesions present; neoplasia; majority of cases (84%) | Remove affected segment; end-to-end anastomosis with sutures (absorbable monofilament) or staples |
| Enteroplication | Prevention of recurrence; recurrent intussusception; hyperperistalsis at surgery; idiopathic cases; spontaneous reduction | Adjacent intestinal loops sutured together from duodenocolic ligament to ileum; prevents re-telescoping |
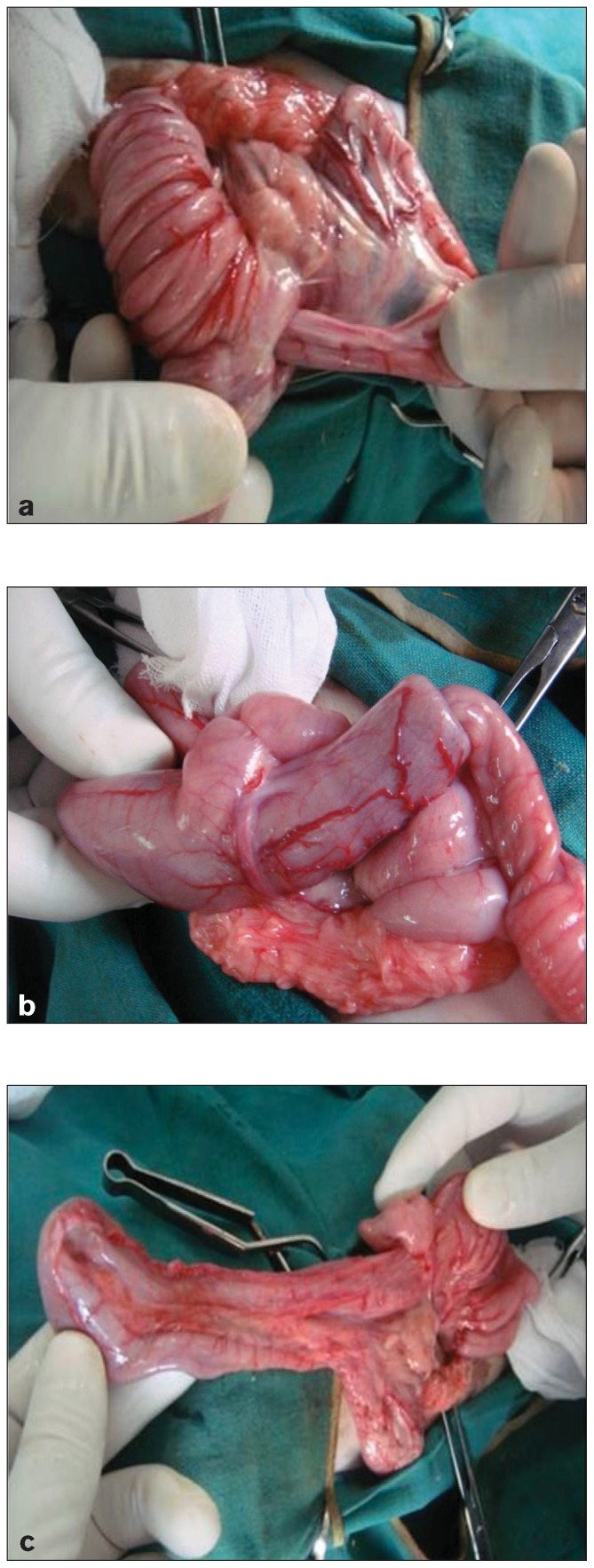
Figure 4. Intraoperative photograph showing an intussusception at exploratory laparotomy, demonstrating the telescoped segment of bowel prior to surgical correction.
Surgical Decision Making
Assessment of bowel viability is critical. Signs of viable bowel include: pink color, presence of peristalsis, pulsatile mesenteric vessels, and return of color after decompression. Non-viable bowel appears dark purple/black, lacks peristalsis, and has no mesenteric pulses - these segments require resection.
High-Yield Note: Enteroplication is controversial! While it may prevent recurrence (recurrence rate 0% with enteroplication vs. up to 28% without in some studies), it can cause serious complications including intestinal obstruction from vegetative material and strangulation of enteroplicated loops. The decision to perform enteroplication should be weighed against these risks. Consider it for: recurrent intussusception, visible hyperperistalsis at surgery, spontaneous reduction cases, and idiopathic cases in young dogs.
Postoperative Care
- Continued IV fluid therapy: Until eating normally
- Analgesia: Opioids (also provide GI motility benefits)
- Antiemetics: As needed
- Antibiotics: Depending on contamination level
- Early enteral nutrition: Small, frequent meals of highly digestible food within 12-24 hours if tolerated
- Treat underlying cause: Deworming, continue parvovirus treatment, address dietary issues
- Monitor for recurrence: Most recurrences occur within 72 hours to 3 weeks postoperatively
Prognosis and Complications
Prognosis
With appropriate surgical treatment, prognosis is generally good. Survival rates with surgical correction range from 70-90% depending on underlying cause and timing of intervention. Factors affecting prognosis include:
- Duration of intussusception (better if treated early)
- Underlying cause (parvovirus carries higher mortality)
- Presence/absence of peritonitis
- Amount of bowel resected
- Prevention of recurrence
Complications
| Complication | Notes |
|---|---|
| Recurrence | 3-25% without enteroplication; usually within 72 hours to 3 weeks; occurs proximal to original site |
| Dehiscence/Anastomotic Leakage | Most common surgical complication; leads to septic peritonitis; typically occurs 3-5 days post-op |
| Septic Peritonitis | From bowel necrosis/perforation or anastomotic dehiscence; high mortality |
| Short Bowel Syndrome | If extensive resection required; malabsorption, diarrhea, weight loss |
| Enteroplication Complications | Intestinal obstruction, strangulation, abscess formation, abdominal discomfort |
| Postoperative Ileus | Temporary decreased GI motility; managed with prokinetics if needed |
Board Tip - Recurrence Prevention: "TRAP" prevents recurrence: Treat the underlying cause (deworm, treat enteritis) Resect non-viable bowel (don't just reduce if damaged) Assess for enteroplication (selective cases) Prevent parasites/parvovirus with routine preventive care
Differential Diagnosis
When a young dog presents with vomiting, bloody diarrhea, and abdominal pain, consider:
- Parvoviral enteritis - can be concurrent with intussusception
- Intestinal foreign body obstruction
- Hemorrhagic gastroenteritis (HGE)
- Intestinal volvulus/mesenteric torsion
- Severe parasitism
- Intestinal neoplasia (especially in older dogs)
- Rectal prolapse - distinguish from prolapsed intussusception
Summary - Key Takeaways
- Definition: Invagination of one intestinal segment (intussusceptum) into an adjacent segment (intussuscipiens)
- Most common location: Ileocolic junction
- Signalment: 75% of cases occur in dogs less than 1 year of age
- Major predisposing factor: Any cause of enteritis, especially canine parvovirus and parasites
- Classic clinical signs: Vomiting, bloody diarrhea, palpable abdominal mass, abdominal pain
- Diagnostic gold standard: Abdominal ultrasound showing TARGET SIGN (pathognomonic)
- Treatment: SURGICAL - resection and anastomosis in most cases (84%); consider enteroplication for recurrence prevention
- Recurrence rate: 3-25% without enteroplication, usually within 72 hours to 3 weeks
- Prognosis: Good with early surgical intervention (70-90% survival)
Practice Question
| A 5-month-old intact male German Shepherd is presented for acute onset of vomiting, bloody diarrhea, and lethargy of 2 days duration. The puppy was acquired from a shelter 1 week ago and is unvaccinated. On physical examination, the dog is 8% dehydrated with a heart rate of 160 bpm, pale mucous membranes, and a palpable tubular mass in the mid-abdomen. An abdominal ultrasound reveals dilated fluid-filled small intestinal loops and a multi-layered structure with alternating hyperechoic and hypoechoic concentric rings in the right cranial quadrant. What is the most appropriate next step in management? A. Administer barium contrast and repeat radiographs in 2 hours B. Start IV fluid therapy and proceed to exploratory laparotomy C. Administer metoclopramide and monitor for 24 hours D. Perform colonoscopy to visualize the intussusception E. Attempt hydrostatic reduction using a barium enema |
|---|
Correct Answer: B
Explanation
Option B is correct. The ultrasound findings of concentric rings (target sign) are pathognomonic for intussusception. Combined with the clinical presentation (young, unvaccinated dog with vomiting, bloody diarrhea, palpable abdominal mass), this confirms the diagnosis. Intussusception is a surgical emergency. The patient should be stabilized with IV fluid therapy to correct dehydration and electrolyte abnormalities, and then proceed to exploratory laparotomy for surgical correction. Delays increase the risk of bowel necrosis and peritonitis.
Option A (barium contrast) is incorrect because the diagnosis has already been made with ultrasound. Barium contrast would delay definitive treatment and is unnecessary. Additionally, barium is contraindicated if perforation is suspected.
Option C (metoclopramide and monitoring) is incorrect because intussusception requires surgical intervention. Prokinetic agents and conservative management will not resolve the problem and delays worsen prognosis.
Option D (colonoscopy) is incorrect because colonoscopy is not standard for diagnosing or treating intussusception in dogs. The diagnosis is already confirmed with ultrasound.
Option E (hydrostatic reduction) is incorrect. While hydrostatic reduction is commonly used in pediatric human medicine, it is not standard of care in veterinary patients. In veterinary medicine, surgical exploration allows assessment of bowel viability and treatment of underlying causes.
High-Yield Note: When you see a young, unvaccinated dog with acute GI signs and a TARGET SIGN on ultrasound, think intussusception and proceed to surgery after stabilization. Remember this puppy is also at high risk for parvovirus given the signalment and shelter origin - test for parvovirus and provide appropriate supportive care, but do not delay surgery for the intussusception. The intussusception may have developed as a complication of parvoviral enteritis.
Image Sources
Figure 2 - Ultrasound triple circle/target sign (transverse and longitudinal views, double intussusception, Case 1): Aprea F et al. (2012). "Ultrasonographic diagnosis and surgical management of double intestinal intussusception in 3 dogs." Can Vet J. Figure 2. PMC3398523. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC3398523/ - Open Access.
Figure 3 - Lateral radiograph showing gas-distended intestinal loops (Case 2, double intussusception): Aprea F et al. (2012). Can Vet J. Figure 1. PMC3398523. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC3398523/ - Open Access.
Figure 4 - Intraoperative photograph of double jejunoileal intussusception through ileocolic orifice prior to surgical correction (Case 1): Aprea F et al. (2012). Can Vet J. Figure 3. PMC3398523. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC3398523/ - Open Access.
References
- American College of Veterinary Surgeons. Intussusception. Available at: https://www.acvs.org/small-animal/intussusception/
- Applewhite AA, Hawthorne JC, Cornell KK. Complications of enteroplication for the prevention of intussusception recurrence in dogs: 35 cases (1989-1999). J Am Vet Med Assoc. 2001;219:1415-1418.
- Chagnon Larose P, et al. Clinical findings and outcomes of 153 dogs surgically treated for intestinal intussusceptions. Vet Surg. 2020;49:858-867.
- Levitt L, Bauer MS. Intussusception in dogs and cats: A review of 36 cases. Can Vet J. 1992;33:660-664.
- Merck Veterinary Manual. Canine Parvovirus Infection. Available at: https://www.msdvetmanual.com/digestive-system/
- Oakes MG, Lewis DD, Hosgood G, Beale BS. Enteroplication for the prevention of intussusception recurrence in dogs: 31 cases (1978-1992). J Am Vet Med Assoc. 1994;205:72-75.
- Patsikas MN, et al. Acute enteritis or gastroenteritis in young dogs as a predisposing factor for intestinal intussusception: a retrospective study. J Vet Med A. 2003;50:416-420.
- Patsikas MN, Papazoglou LG. Current Views in the Diagnosis and Treatment of Intestinal Intussusception. Topics in Companion Animal Medicine. 2019;35:28-35.
- VCA Animal Hospitals. Intussusception in Dogs. Available at: https://vcahospitals.com/know-your-pet/intussusception-in-dogs
- WSAVA 2008 Congress. Intussusception: Diagnosis and Treatment. Available at: https://www.vin.com/
Practice NAVLE Questions
Test your knowledge with 10,000+ exam-style questions, detailed explanations, and timed exams.
Start Your Free Trial →