Canine Diabetes Insipidus Study Guide
Canine Diabetes Insipidus Study Guide
NAVLE & BCSE Examination Preparation
Endocrine System | Species: Canine
Estimated Read Time: 30-35 minutes | Last Updated: December 2024
Overview and Clinical Importance
Diabetes insipidus (DI) is a rare endocrine disorder characterized by the production of large volumes of dilute urine and compensatory polydipsia. Unlike diabetes mellitus, which involves abnormal glucose metabolism, diabetes insipidus results from dysfunction in the antidiuretic hormone (ADH) pathway. The term "insipidus" derives from Latin meaning "tasteless," referring to the dilute, tasteless urine produced by affected patients, in contrast to the sweet urine of diabetes mellitus.
Understanding diabetes insipidus is essential for NAVLE success because it requires differentiation from numerous other causes of polyuria and polydipsia, a common clinical presentation in small animal practice. The condition demonstrates fundamental concepts in endocrine physiology, renal function, and diagnostic reasoning.
High-Yield Note: Diabetes insipidus is RARE compared to other causes of PU/PD. On board exams, always rule out more common differentials first: diabetes mellitus, chronic kidney disease, hyperadrenocorticism, pyometra, hyperthyroidism (cats), and hypercalcemia.
Learning Objectives
- Differentiate central diabetes insipidus (CDI) from nephrogenic diabetes insipidus (NDI) based on pathophysiology and clinical presentation
- Understand the physiologic role of antidiuretic hormone (ADH/vasopressin) in water homeostasis
- Interpret diagnostic test results including urine specific gravity, water deprivation test, and desmopressin trial
- Select appropriate treatment protocols for CDI versus NDI
- Recognize breed predispositions and common etiologies for diabetes insipidus in dogs
Pathophysiology of Diabetes Insipidus
Normal ADH Physiology
Antidiuretic hormone (ADH), also known as arginine vasopressin (AVP), is a nonapeptide hormone synthesized in the supraoptic and paraventricular nuclei of the hypothalamus. The hormone is transported along axons through the infundibular stalk and stored in the posterior pituitary gland (neurohypophysis) until release.
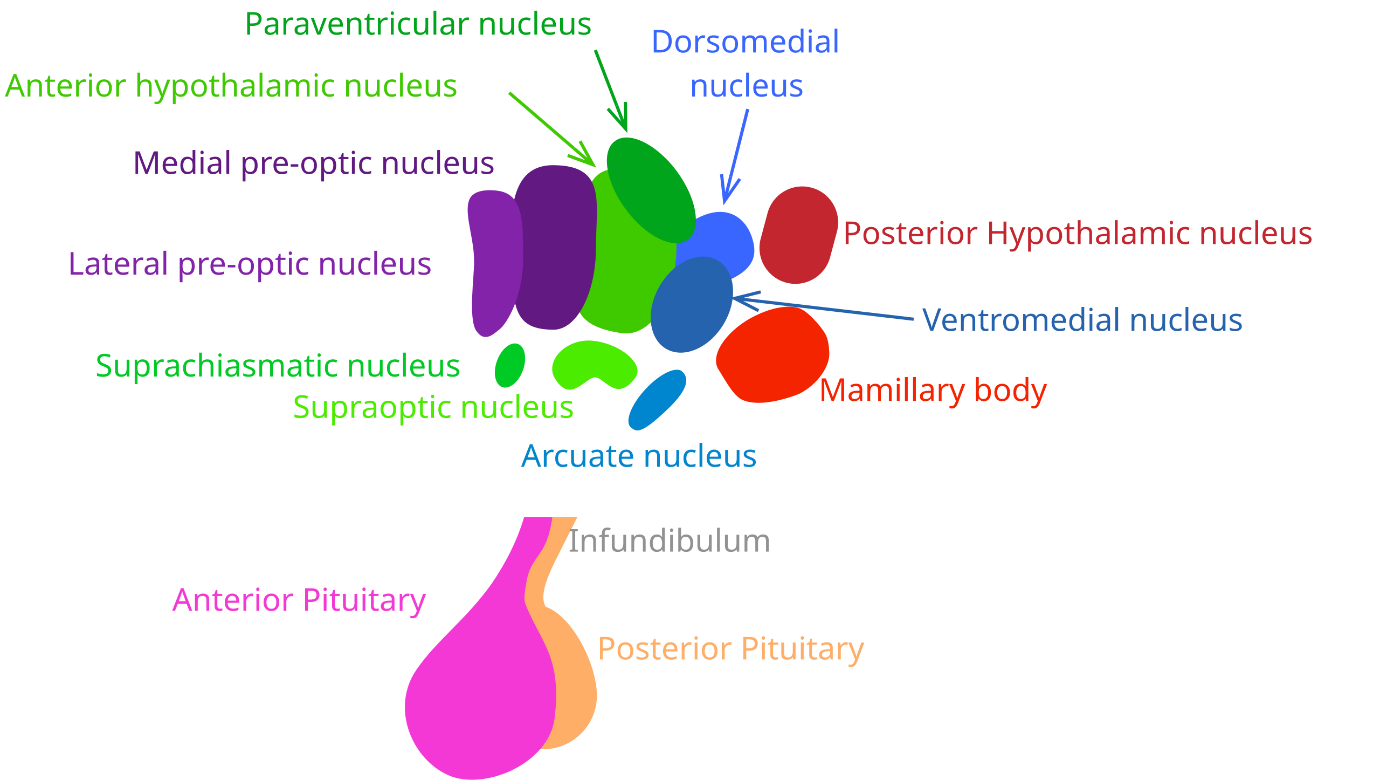
Diagram showing the hypothalamic-pituitary axis with ADH synthesis in the supraoptic and paraventricular nuclei and release from the posterior pituitary (Figure 1)
ADH release is triggered by:
- Increased plasma osmolality (detected by hypothalamic osmoreceptors)
- Decreased blood volume or pressure (detected by baroreceptors)
- Angiotensin II stimulation
Mechanism of Action: ADH binds to V2 receptors on the basolateral membrane of principal cells in the renal collecting duct. This activates adenylate cyclase, increasing intracellular cAMP, which activates protein kinase A. The cascade leads to insertion of aquaporin-2 (AQP2) water channels into the apical membrane, dramatically increasing water permeability and allowing water reabsorption from the tubular lumen into the hypertonic medullary interstitium.
Board Tip: Remember the ADH pathway with "HIPS": Hypothalamus (synthesis) → Infundibulum (transport) → Posterior Pituitary (storage) → Second messengers in kidney (action). Disruption anywhere along this pathway can cause diabetes insipidus.
Classification of Diabetes Insipidus
Central Diabetes Insipidus (CDI)
Central diabetes insipidus results from partial or complete deficiency of ADH synthesis or secretion. At least 80-90% of ADH-producing neurons must be destroyed before clinical signs become apparent.
Etiologies of CDI:
- Idiopathic: Most common cause; may represent undetected autoimmune destruction
- Neoplasia: Pituitary tumors (approximately 40% of CDI cases), craniopharyngioma, pituitary chromophobe adenoma/adenocarcinoma, metastatic tumors
- Trauma: Head injury, skull fractures (may cause transient or permanent CDI)
- Congenital malformations: Pituitary cysts, hypothalamic-pituitary malformations
- Inflammatory/Infectious: Lymphocytic hypophysitis, granulomatous disease, encephalitis
- Iatrogenic: Post-hypophysectomy (common complication)
Nephrogenic Diabetes Insipidus (NDI)
Nephrogenic diabetes insipidus occurs when the kidneys fail to respond appropriately to ADH despite normal or elevated plasma ADH concentrations. NDI can be primary (congenital) or secondary (acquired).
Primary (Congenital) NDI:
- Rare congenital defect in V2 receptor or aquaporin-2 channels
- Clinical signs typically appear by 8-12 weeks of age
- Breed predispositions: German Shepherds, Miniature Poodles, Siberian Huskies
Secondary (Acquired) NDI - More Common:
- Chronic kidney disease (CKD)
- Hypercalcemia
- Hypokalemia
- Hyperadrenocorticism (cortisol antagonizes ADH action)
- Pyometra/endotoxemia
- Pyelonephritis
- Leptospirosis
- Drugs (glucocorticoids, certain antibiotics)
- Hepatic disease
Comparison: CDI vs NDI
| Feature | Central DI (CDI) | Nephrogenic DI (NDI) |
|---|---|---|
| Defect Location | Hypothalamus/Pituitary | Kidney (collecting duct) |
| ADH Levels | Low to absent | Normal to elevated |
| Desmopressin Response | Positive (USG increases greater than 50%) | Minimal to no response |
| Age at Onset | Middle-aged to senior (most common) | Congenital: less than 1 year; Acquired: any age |
| Treatment | Desmopressin (DDAVP) | Treat underlying cause; Thiazide diuretics; Low-sodium diet |
| Prognosis | Good with lifelong treatment (unless pituitary tumor) | Depends on underlying cause; Congenital NDI is irreversible |
Clinical Presentation
Clinical Signs
The hallmark clinical signs of diabetes insipidus are profound polyuria (PU) and polydipsia (PD). These signs can be dramatic and often bring the patient to clinical attention.
Key Clinical Features:
- Polyuria: Urine production greater than 50 mL/kg/day (normal: 20-45 mL/kg/day)
- Polydipsia: Water consumption greater than 100 mL/kg/day (normal: 20-70 mL/kg/day)
- Extreme water consumption: May exceed 200-800 mL/kg/day in severe cases
- Urinary incontinence (due to bladder distension from urine volume)
- Nocturia (urination at night)
- House soiling (previously house-trained dogs)
- Dehydration (if water access is restricted)
- Weight loss (occasionally, due to preoccupation with drinking)
Exam Focus: CRITICAL - Dogs with complete DI can become severely dehydrated within 4-6 hours if water is withheld. This is clinically important for hospitalized patients and before anesthesia. Always ensure free water access is available.
Physical Examination Findings
Physical examination is often unremarkable in uncomplicated diabetes insipidus. Key findings may include:
- Normal body condition (unless severe dehydration)
- Distended urinary bladder on palpation
- Dehydration signs if water restricted: tacky mucous membranes, prolonged skin tent, sunken eyes
- Neurological signs if pituitary mass effect present: blindness, circling, seizures, behavioral changes
Diagnostic Approach
Initial Diagnostic Workup
The diagnosis of diabetes insipidus requires a systematic approach to first exclude more common causes of PU/PD before pursuing specific testing.
Minimum Database
| Test | Expected Findings in DI / Differential Rule-Outs |
|---|---|
| CBC | Usually normal; May show hemoconcentration if dehydrated |
| Serum Chemistry | Usually normal; Rules out: diabetes mellitus (glucose), CKD (BUN/creatinine), liver disease (ALT, ALP), hypercalcemia (calcium) |
| Urinalysis | Hyposthenuria (USG 1.001-1.006); No glucosuria (rules out DM); No proteinuria or active sediment (rules out CKD, UTI) |
| Urine Culture | Negative; Rules out pyelonephritis |
| Electrolytes | May show hypernatremia if dehydrated; Hypokalemia can cause secondary NDI |
Urine Specific Gravity (USG) Interpretation
| USG Range | Interpretation | Clinical Significance |
|---|---|---|
| Less than 1.008 | Hyposthenuria | Highly suggestive of complete DI (active dilution) |
| 1.008-1.012 | Isosthenuria | Partial DI or early renal disease |
| Greater than 1.030 | Concentrated | Rules out complete DI (normal concentrating ability) |
High-Yield Note: A USG less than 1.008 in a dehydrated patient is HIGHLY suspicious for diabetes insipidus. Normal dogs should be able to concentrate urine above 1.030 when dehydrated. The key finding is persistent hyposthenuria despite physiological stimuli for water conservation.
Desmopressin (DDAVP) Trial - Preferred Diagnostic Test
The desmopressin trial is now the preferred diagnostic approach as it is safer than water deprivation testing and provides both diagnostic and therapeutic information.
Protocol:
- Establish baseline: Owner measures 24-hour water intake for 2-3 days and collects daily urine samples
- Administer desmopressin: 0.1-0.2 mg PO every 8-12 hours OR 1-4 drops (conjunctival) every 12 hours for 5-7 days
- Continue monitoring water intake and urine collection during treatment
- Evaluate response after 5-7 days (allows time to overcome medullary washout)
Interpretation:
- CDI: Greater than 50% decrease in water intake; USG increases significantly (greater than 1.015-1.025)
- NDI: Minimal to no change in water intake or USG
- Partial CDI: Moderate improvement (partial response)
Modified Water Deprivation Test
Note: This test has largely fallen out of favor due to significant risks including severe dehydration, hypernatremia, neurological signs, and potential death in dogs with complete DI. The desmopressin trial is preferred. However, understanding this test is important for board examinations.
Protocol Overview:
- Gradual water restriction over several days prior to test
- Complete water withholding with close monitoring
- Monitor body weight, hydration status, USG every 1-2 hours
- Stop test if: greater than 5% body weight loss, severe dehydration, USG greater than 1.030
- Administer exogenous ADH (desmopressin) and monitor response
Advanced Imaging
If CDI is diagnosed, MRI or CT scan of the brain is recommended to evaluate for pituitary masses. Up to 40% of dogs with CDI have an underlying pituitary tumor.
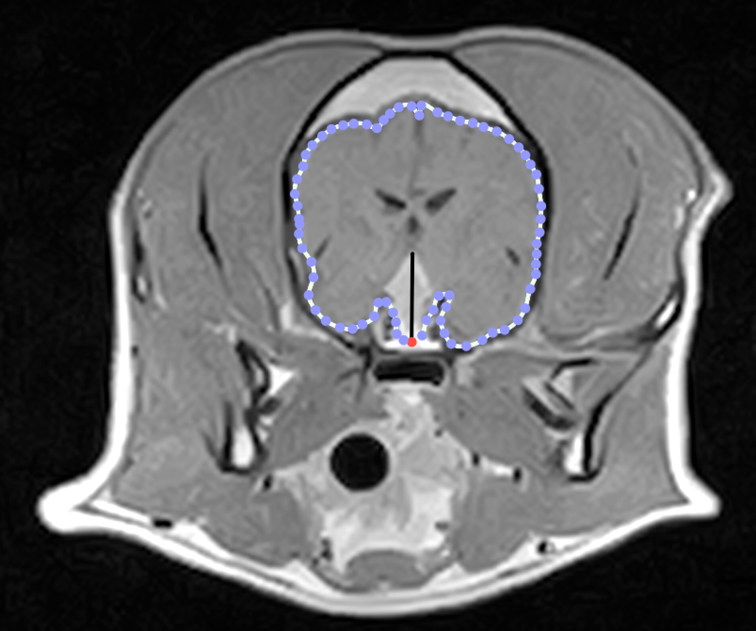
Figure 2: Transverse post-contrast T1-W MR image of the brain from a dog with a DPM.
Reference: Menchetti M, De Risio L, Galli G, Bruto Cherubini G, Corlazzoli D, Baroni M, Gandini G. Neurological abnormalities in 97 dogs with detectable pituitary masses. Vet Q. 2019 Dec;39(1):57-64. doi: 10.1080/01652176.2019.1622819. PMID: 31112462; PMCID: PMC6831018.
Treatment Options
Treatment of Central Diabetes Insipidus
Desmopressin (DDAVP) is the treatment of choice for CDI. It is a synthetic vasopressin analog with potent V2 receptor activity (antidiuretic effect) and minimal V1 activity (vasopressor effect).
Desmopressin Dosing Protocols
| Route | Dosage | Notes |
|---|---|---|
| Conjunctival | 1-4 drops (0.1 mg/mL solution) every 12-24 hours | May cause local irritation; Good absorption |
| Oral Tablets | 0.1-0.2 mg every 8-12 hours | Most convenient; Most expensive; Variable absorption |
| Subcutaneous | 1-5 mcg once or twice daily | Most cost-effective; Requires injection |
| Intranasal | 1-2 drops per nostril every 12-24 hours | Often difficult in dogs |
Monitoring and Dose Adjustment
- Maximal effect occurs 2-8 hours after administration
- Duration of action: 8-24 hours (variable)
- Titrate dose to effect based on water intake and urine output
- Monitor for overhydration: vomiting, diarrhea, neurological signs (hyponatremia)
- DO NOT restrict water access
Treatment of Nephrogenic Diabetes Insipidus
Treatment of NDI is more challenging as the kidneys do not respond to ADH. The primary approach is to treat any underlying cause for acquired NDI.
| Treatment | Mechanism/Notes |
|---|---|
| Thiazide Diuretics | Hydrochlorothiazide (2-4 mg/kg PO BID): Paradoxically reduces urine output by 30-50% through proximal tubular sodium and water reabsorption |
| Low-Sodium Diet | Reduces solute load to kidneys, decreasing obligatory water excretion |
| Free Water Access | CRITICAL - Must always be available to prevent life-threatening dehydration |
| Treat Underlying Cause | Correct hypercalcemia, hypokalemia; Treat hyperadrenocorticism; Discontinue offending drugs |
Board Tip: Remember thiazides work paradoxically in DI: "THIRSTY = Thiazides Help In Reducing Severe Thirst, Yes!" The diuretic effect reduces sodium delivery to the distal nephron, causing compensatory proximal reabsorption of both sodium AND water.
Prognosis
Central Diabetes Insipidus: Prognosis is generally good with lifelong desmopressin therapy, provided there is no underlying pituitary tumor. Dogs can live normal lifespans with appropriate treatment and free water access. If a pituitary tumor is present, prognosis depends on tumor type and size.
Trauma-induced CDI: May be transient (resolving in days to weeks) or permanent. Prophylactic desmopressin post-hypophysectomy can minimize CDI development.
Nephrogenic Diabetes Insipidus: Prognosis varies. Acquired NDI may resolve with treatment of the underlying condition. Congenital NDI is irreversible but can be managed. Quality of life can be significantly impacted by the need for constant water access and frequent urination.
Differential Diagnosis of Polyuria/Polydipsia
Always consider and rule out more common causes of PU/PD before pursuing specific DI diagnostics:
| Condition | Key Distinguishing Features |
|---|---|
| Diabetes Mellitus | Hyperglycemia, glucosuria, HIGH USG (osmotic diuresis) |
| Chronic Kidney Disease | Azotemia, isosthenuria, proteinuria, small kidneys |
| Hyperadrenocorticism | Elevated ALP, stress leukogram, pot-bellied appearance, alopecia |
| Hypercalcemia | Elevated serum calcium, causes secondary NDI |
| Pyometra | Intact female, vaginal discharge, uterine enlargement |
| Psychogenic Polydipsia | Behavioral, CAN concentrate urine when dehydrated, responds to desmopressin |
| Hepatic Disease | Elevated liver enzymes, low BUN, hypoalbuminemia |
| Hypoadrenocorticism | Electrolyte abnormalities (hyponatremia, hyperkalemia), bradycardia |
High-Yield Note: "HARD UP PP" - Common causes of PU/PD: Hyperadrenocorticism, Addison's disease, Renal disease, Diabetes mellitus, Uterus (pyometra), Pyelonephritis, Psychogenic polydipsia. Remember DI only after ruling these out!
Practice Question
| A 6-year-old spayed female Australian Shepherd presents with a 4-month history of progressive polydipsia and polyuria. The owner reports the dog is drinking approximately 2 liters of water daily and frequently needs to urinate at night. Physical examination reveals normal hydration, and the dog appears bright and alert. Initial bloodwork shows: BUN 18 mg/dL (normal), creatinine 1.0 mg/dL (normal), glucose 95 mg/dL (normal), calcium 10.2 mg/dL (normal), ALT 45 U/L (normal), ALP 85 U/L (normal). Urinalysis reveals a USG of 1.004, no glucosuria, no proteinuria, and inactive sediment. Urine culture is negative. A desmopressin trial is initiated. After 7 days of treatment with desmopressin (0.1 mg PO q12h), the owner reports a dramatic decrease in water intake, and a urine sample now shows a USG of 1.022. What is the most appropriate next step in managing this patient? A. Discontinue desmopressin and monitor B. Continue desmopressin therapy and perform brain MRI/CT C. Switch to thiazide diuretic therapy D. Perform a water deprivation test E. Start chlorpropamide therapy |
|---|
Correct Answer: B
Explanation
Central diabetes insipidus (CDI) is the correct diagnosis based on the clinical presentation and positive response to desmopressin. The dramatic improvement in water intake and increased urine concentration (from 1.004 to 1.022) after desmopressin administration confirms ADH deficiency characteristic of CDI. The next step is to continue lifelong desmopressin therapy AND perform advanced brain imaging (MRI or CT) because approximately 40% of dogs with CDI have an underlying pituitary tumor. Early detection of a mass allows for treatment planning and prognostic assessment.
Option A (Discontinue desmopressin) is incorrect because CDI requires lifelong treatment. Discontinuing therapy would result in recurrence of severe PU/PD.
Option C (Thiazide diuretics) is incorrect because thiazide diuretics are used for nephrogenic DI, not CDI. This patient responded to desmopressin, indicating ADH deficiency (central cause).
Option D (Water deprivation test) is incorrect because the desmopressin trial has already provided diagnostic information. Water deprivation testing is riskier and would not provide additional useful information at this point.
Option E (Chlorpropamide) is incorrect because chlorpropamide is an older, less effective treatment that works by potentiating endogenous ADH. Desmopressin is the preferred treatment for CDI.
High-Yield Note: For board exams, remember the key diagnostic feature: A positive response to desmopressin (greater than 50% decrease in water intake + increased USG) = Central DI. No response to desmopressin = Nephrogenic DI. Always recommend brain imaging for confirmed CDI to rule out pituitary masses.
Summary - Key Takeaways
- Diabetes insipidus is RARE - always rule out more common causes of PU/PD first (DM, CKD, HAC, pyometra, hypercalcemia)
- Two types: CDI (ADH deficiency) and NDI (kidney unresponsive to ADH)
- Hallmark finding: Hyposthenuria (USG less than 1.008) that persists despite dehydration
- Desmopressin trial is the preferred diagnostic test (safer than water deprivation)
- CDI: Responds to desmopressin; Treat with lifelong DDAVP; Image brain for pituitary tumors
- NDI: Does NOT respond to desmopressin; Treat underlying cause; Use thiazides and low-sodium diet
- CRITICAL: Never restrict water in DI patients - can cause fatal dehydration within hours
- Prognosis: Generally good with appropriate treatment; depends on underlying cause
Image Sources
- Figure 1 - Hypothalamic-Pituitary Axis Diagram: Wikimedia Commons - "Hypothalamus and Pituitary.svg" - Creative Commons Attribution-Share Alike 4.0 International license. URL: https://commons.wikimedia.org/wiki/File:Hypothalamus_and_Pituitary.svg
- Figure 3 - Pituitary MRI: PMC Open Access - Menchetti M, De Risio L, Galli G, Bruto Cherubini G, Corlazzoli D, Baroni M, Gandini G. Neurological abnormalities in 97 dogs with detectable pituitary masses. Vet Q. 2019 Dec;39(1):57-64. doi: 10.1080/01652176.2019.1622819. PMID: 31112462; PMCID: PMC6831018.
References
- Merck Veterinary Manual. Diabetes Insipidus in Animals. 2024. Available at: https://www.merckvetmanual.com/endocrine-system/the-pituitary-gland/diabetes-insipidus-in-animals
- Nelson RW, Feldman EC. Canine and Feline Endocrinology and Reproduction. 4th ed. Elsevier/Saunders; 2015.
- Harb MF, Nelson RW, Feldman EC, et al. Central diabetes insipidus in dogs: 20 cases (1986-1995). J Am Vet Med Assoc. 1996;209(11):1884-1888.
- Peralta J, Labato MA. Central diabetes insipidus. Clinician's Brief. June 2019.
- Takemura N. Successful long-term treatment of congenital nephrogenic diabetes insipidus in a dog. J Small Anim Pract. 1998;39(12):592-594.
- Cohen M, Post GS. Water transport in the kidney and nephrogenic diabetes insipidus. J Vet Intern Med. 2002;16(5):510-517.
- VCA Animal Hospitals. Diabetes Insipidus in Dogs. Available at: https://vcahospitals.com/know-your-pet/diabetes-insipidus-in-dogs
- Ettinger SJ, Feldman EC. Textbook of Veterinary Internal Medicine. 8th ed. Elsevier Saunders; 2017.
Practice NAVLE Questions
Test your knowledge with 10,000+ exam-style questions, detailed explanations, and timed exams.
Start Your Free Trial →