Canine Systemic Hypertension Study Guide
Canine Systemic Hypertension Study Guide
NAVLE Study Guide
Cardiovascular System | Species: Canine
Estimated Read Time: 30-35 minutes | Last Updated: December 2024
Overview and Clinical Importance
Systemic hypertension is defined as a sustained elevation in systemic arterial blood pressure that increases the risk of target organ damage (TOD). In dogs, systemic hypertension is predominantly a secondary condition, occurring as a consequence of an underlying disease process. Unlike humans, primary (idiopathic or essential) hypertension is rare in dogs, accounting for less than 20% of cases.
The most vulnerable organ systems affected by sustained hypertension include the eyes, kidneys, heart, and brain. Target organ damage can lead to devastating consequences including acute blindness, progressive renal injury, left ventricular hypertrophy, and neurological dysfunction. The rationale for treating hypertension is to minimize or prevent these injuries.
Understanding the pathophysiology, diagnosis, and management of canine hypertension is essential for the NAVLE, as it frequently appears in clinical scenario questions involving geriatric dogs with concurrent endocrine or renal disease.
Learning Objectives
- Define systemic hypertension and understand the ACVIM blood pressure classification system
- Identify the primary causes of secondary hypertension in dogs
- Recognize clinical signs and target organ damage associated with hypertension
- Master blood pressure measurement techniques and interpretation
- Apply appropriate pharmacological treatment protocols for canine hypertension
Definition and Classification
According to the 2018 ACVIM Consensus Statement, systemic hypertension is classified based on systolic blood pressure (SBP) measurements and the associated risk of target organ damage. The classification system helps guide treatment decisions.
ACVIM Blood Pressure Classification (2018)
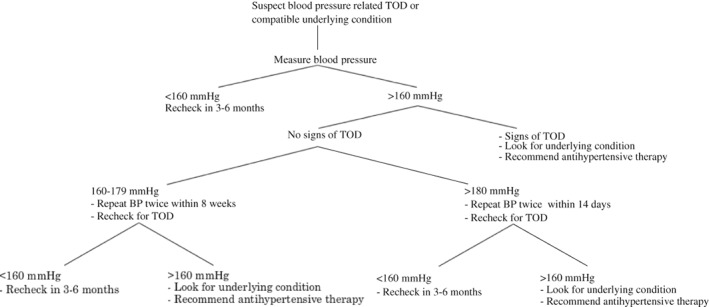
Figure 1 - The recommended approach to the evaluation of a possibly hypertensive patient.
Reference: Acierno MJ, Brown S, Coleman AE, Jepson RE, Papich M, Stepien RL, Syme HM. ACVIM consensus statement: Guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats. J Vet Intern Med. 2018 Nov;32(6):1803-1822. doi: 10.1111/jvim.15331. Epub 2018 Oct 24. PMID: 30353952; PMCID: PMC6271319.
| Category | SBP (mm Hg) | TOD Risk | Clinical Action |
|---|---|---|---|
| Normotensive | Less than 140 | Minimal | Routine monitoring |
| Prehypertensive | 140-159 | Low | Recheck in 1-2 months |
| Hypertensive | 160-179 | Moderate | Confirm; treat if TOD present |
| Severely Hypertensive | 180 or greater | High | Initiate treatment promptly |
High-Yield Note: For NAVLE purposes, remember that SBP greater than or equal to 160 mm Hg is considered hypertensive, and SBP greater than or equal to 180 mm Hg requires prompt treatment initiation. Treatment should begin after a single measurement session if active target organ damage is present.
Etiology: Causes of Canine Hypertension
Canine hypertension is categorized as either primary (idiopathic) or secondary. Secondary hypertension is far more common in dogs, accounting for approximately 80% of cases.
Primary (Idiopathic) Hypertension
Primary hypertension, also called essential hypertension, is diagnosed when no identifiable underlying cause can be found. This is relatively rare in dogs compared to humans. Some studies suggest dogs may be resistant to developing primary hypertension. Diagnosis requires ruling out all secondary causes through comprehensive diagnostic testing.
Secondary Hypertension
The following conditions are the most common causes of secondary hypertension in dogs:
| Disease | Mechanism | Prevalence of Hypertension |
|---|---|---|
| Chronic Kidney Disease (CKD) | RAAS activation, sodium retention, decreased GFR, volume overload | 31-93% of dogs with CKD |
| Hyperadrenocorticism (Cushing's) | Cortisol-induced sodium retention, increased vascular sensitivity to catecholamines | 59-86% of affected dogs |
| Pheochromocytoma | Excessive catecholamine secretion causing vasoconstriction | Up to 86% (often episodic) |
| Diabetes Mellitus | Diabetic nephropathy, vascular changes, insulin resistance | 24-46% of diabetic dogs |
| Hyperaldosteronism | Sodium retention and potassium wasting | Rare but significant |
| Glomerulonephritis | Protein loss, RAAS activation, glomerular damage | Common with proteinuria |
| Obesity | Increased sympathetic tone, RAAS activation, insulin resistance | Variable; contributes to risk |
Board Tip: The "Big Three" causes of secondary hypertension in dogs are: (1) Chronic Kidney Disease, (2) Hyperadrenocorticism (Cushing's disease), and (3) Diabetes Mellitus. When a NAVLE question presents a hypertensive dog, always look for clues pointing to these underlying conditions!
Memory Aid: "CKD-HAD Hypertension"
C = Chronic Kidney Disease (most common) K = Kidney (Glomerulonephritis) D = Diabetes Mellitus H = Hyperadrenocorticism A = Aldosteronism (Hyperaldosteronism) D = Dangerous tumor (Pheochromocytoma)
Target Organ Damage (TOD)
Sustained hypertension damages organs with extensive microvascular networks. The eyes, kidneys, heart, and brain are the primary targets. Recognizing signs of TOD is critical for both diagnosis and determining the urgency of treatment.
Ocular Target Organ Damage
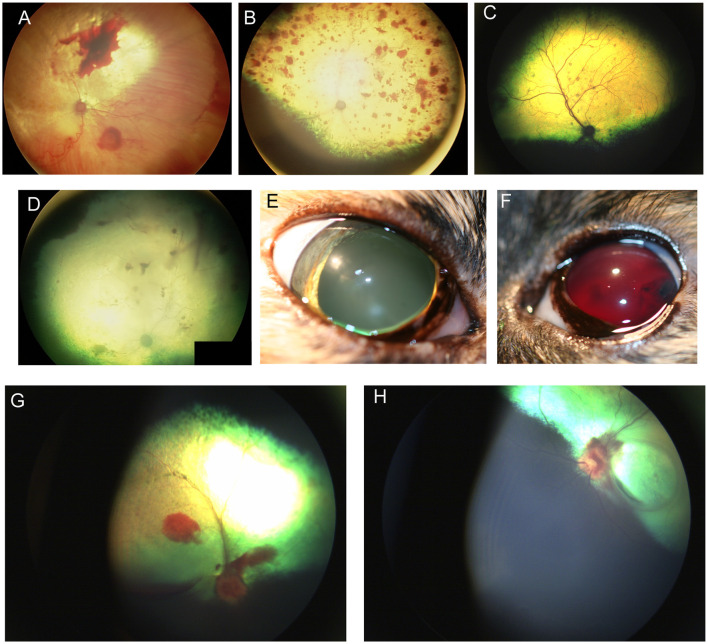
Figure 2 - Hypertensive Retinopathy showing retinal hemorrhage and detachment. (A) Subalbinotic fundus of the right eye of a cat manifesting with subretinal and intraretinal (punctate) hemorrhages of unknown etiology. Tapetal hyperreflectivity and vascular attenuation are also visible. (B–F) Feline hypertensive retinopathy. (B) Multifocal retinal hemorrhages ranging in size from punctate to one optic nerve in diameter, along with tapetal hyperreflectivity and vascular attenuation. Upon presentation the patient had a systolic blood pressure of 215 mmHg and a hematocrit of 20 and a prolonged aPTT at 89.6s (Ref 23.6–54.9s). The cat later became blind and recumbent. Humane euthanasia was elected and a necropsy showed chronic renal failure and a cerebellar hemorrhage. (C) Multifocal punctate retinal hemorrhages and retinal lesions. This cat was diagnosed with a functional adrenal carcinoma and secondary hyperaldosteronism and a systolic blood pressure of 300 mmHg. (D) Right fundus, (E) right eye, and (F) left eye of a cat suffering from hypertensive retinopathy in the right eye, and hypertensive oculopathy in the left. (D) the fundic vasculature is greatly attenuated and the retina is hyporeflective. There are punctate intra-retinal hemorrhages, subretinal and vitreal hemorrhages. (E) the pupil is dilated and non-responsive to light. (F) Hyphema and blood clots are formed in the anterior chamber. (G) Optic neuritis, subretinal and vitreal hemorrhage in the right eye of a dog affected by immune mediated thrombocytopenia. (H) Optic neuritis with flame shaped hemorrhages tracking along the nerve fiber layer, subretinal hemorrhages and focal retinal atrophy in the left eye of the same dog.
Reference: https://pmc.ncbi.nlm.nih.gov/articles/PMC10912207/
Ocular lesions are common in hypertensive dogs and may present as the primary clinical complaint. When SBP exceeds approximately 180 mm Hg, retinal vessels become damaged and may leak or rupture. Key ocular findings include:
- Hypertensive retinopathy: Retinal hemorrhages, vessel tortuosity, arterial narrowing (beading), retinal edema
- Hypertensive choroidopathy: Serous or exudative retinal detachment (bullous detachment)
- Hyphema: Blood in the anterior chamber
- Secondary glaucoma: From anterior uveitis or hyphema
- Acute blindness: Often the presenting complaint; may be sudden onset
High-Yield Note: Acute-onset blindness due to retinal detachment or intraocular hemorrhage is often the first clinical sign noticed by owners. In any dog presenting with sudden blindness, measure blood pressure immediately! If treated promptly, vision may be recoverable in some cases.
Renal Target Organ Damage
Hypertension can both cause and result from kidney disease, creating a vicious cycle. Elevated glomerular capillary pressure leads to:
- Progressive glomerulosclerosis
- Proteinuria (increased UPC ratio)
- Accelerated decline in GFR
- Progression of azotemia
The severity of proteinuria often correlates with the magnitude of hypertension. In dogs with CKD, hypertension is associated with shorter survival times and more rapid disease progression.
Cardiac Target Organ Damage
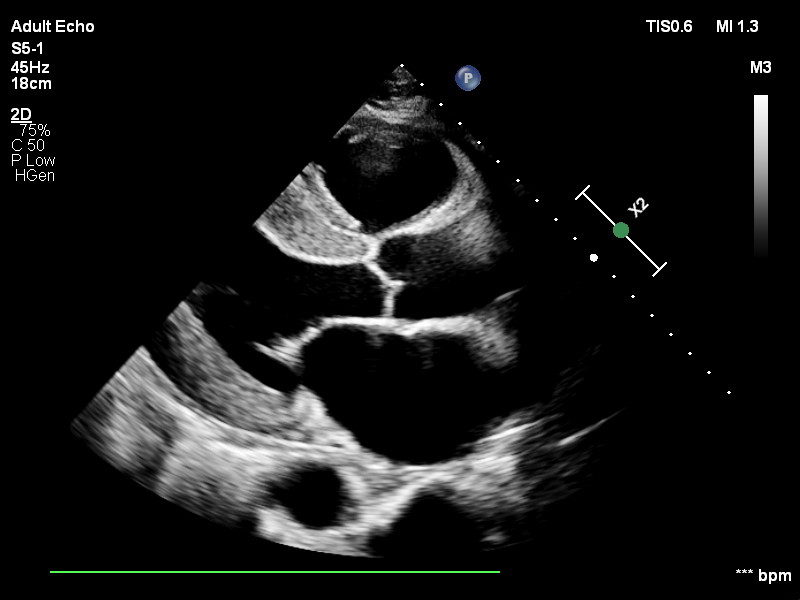
Figure 3 - Echocardiogram showing left ventricular hypertrophy.
Reference - Case courtesy of Karen Machang'a, https://radiopaedia.org/?lang=us - Radiopaedia.org. From the https://radiopaedia.org/cases/187225?lang=us
The heart must work against elevated arterial pressure (increased afterload), leading to compensatory changes:
- Left ventricular hypertrophy (LVH): Concentric hypertrophy to maintain wall stress
- Systolic heart murmur: From dynamic outflow obstruction or concurrent mitral regurgitation
- Gallop rhythm (S4): Indicates reduced ventricular compliance
- Arrhythmias: Ventricular ectopy or atrial fibrillation
- Epistaxis: Nasal vessel rupture from elevated pressure
Neurological Target Organ Damage (Hypertensive Encephalopathy)
Severe hypertension can overwhelm cerebral autoregulation, leading to cerebral edema, hemorrhage, or ischemia. Clinical signs include:
- Seizures
- Altered mentation (disorientation, obtundation, stupor)
- Vestibular signs (head tilt, nystagmus, ataxia)
- Focal neurological deficits
- Sudden collapse
Summary: Target Organ Damage by System
| Organ System | Clinical Signs | Diagnostic Findings |
|---|---|---|
| Eyes | Sudden blindness, mydriasis, hyphema | Retinal hemorrhage, detachment, vessel tortuosity |
| Kidneys | PU/PD, weight loss, vomiting | Azotemia, proteinuria (increased UPC), elevated SDMA |
| Heart | Exercise intolerance, cough, murmur, epistaxis | LVH on echo, gallop rhythm, arrhythmias |
| Brain | Seizures, altered mentation, vestibular signs | MRI: cerebral edema, hemorrhage, infarct |
Diagnosis of Systemic Hypertension
Blood Pressure Measurement Techniques

Figure 4 - Doppler blood pressure measurement technique in a dog.
Image credit: Today's Veterinary Practice
The diagnosis of systemic hypertension is based on reliable blood pressure measurements. The gold standard is direct arterial catheterization, but this is impractical for routine screening. Indirect methods are used clinically:
| Method | Advantages | Limitations |
|---|---|---|
| Doppler Ultrasonography | Accurate in small patients, detects low-pressure states, reliable for SBP | Only measures SBP reliably; requires training; may underestimate values |
| Oscillometry | Automated; provides SBP, DBP, and MAP; minimal training needed | Less reliable in small dogs; affected by movement; may be inaccurate at extremes |
| High-Definition Oscillometry | Improved accuracy over standard oscillometry; pressure waveform visualization | More expensive; requires computer connection for waveform analysis |
ACVIM Recommended Protocol for BP Measurement
- Environment: Quiet, isolated room away from other animals; owner present when possible
- Acclimation: Allow 5-10 minutes for patient to calm before measurement
- Positioning: Sternal or lateral recumbency; minimize vertical distance from heart to cuff
- Cuff selection: Width should be 30-40% of limb/tail circumference at cuff site
- Cuff placement: Forelimb (proximal to carpus), hindlimb (proximal to hock), or tail base
- Measurements: Discard first reading; obtain 5-7 consecutive consistent measurements
- Recording: Document cuff size, site, patient position, technician name, and all values
High-Yield Note: An incorrectly sized cuff is the most common source of error in BP measurement! A cuff that is too small will overestimate BP, while a cuff that is too large will underestimate BP. Always use a cuff width that is 30-40% of the limb circumference.
Situational (White Coat) Hypertension
Anxiety or excitement from the veterinary visit can cause transient BP elevation (situational hypertension). This can lead to misdiagnosis of true pathologic hypertension. To minimize this: measure BP before other procedures, use consistent technique and personnel, allow adequate acclimation time, and confirm elevated readings on at least 2-3 separate occasions before diagnosing hypertension (unless TOD is present).
When to Screen for Hypertension
- Patients with clinical signs consistent with target organ damage
- Dogs with diseases commonly associated with secondary hypertension (CKD, Cushing's, DM)
- Senior dogs (greater than 9 years) as part of wellness screening
- Patients on medications that may affect BP
- Any patient with unexplained acute blindness, epistaxis, or neurological signs
Treatment of Canine Systemic Hypertension
The primary goals of antihypertensive therapy are to: (1) reduce SBP to less than 160 mm Hg (ideally less than 140 mm Hg), (2) prevent or reverse target organ damage, and (3) treat the underlying cause when possible.
Treatment Indications
- SBP greater than or equal to 180 mm Hg: Initiate treatment after single measurement session
- SBP 160-179 mm Hg with TOD: Initiate treatment
- SBP 160-179 mm Hg without TOD: Confirm on 2-3 occasions within 1-2 weeks before treating
- Hypertensive emergency (SBP greater than 200 mm Hg with acute TOD): Immediate treatment required
Pharmacological Therapy
In dogs, systemic hypertension appears to be primarily due to constriction of systemic arterioles. Therefore, potent arterial vasodilators are the most effective antihypertensive agents.
Antihypertensive Medications for Dogs
| Drug | Class | Dosage | Notes |
|---|---|---|---|
| Amlodipine | Calcium Channel Blocker (CCB) | 0.1-0.5 mg/kg PO q12-24h | First-line in dogs; potent arteriolar dilator; may cause gingival hyperplasia |
| Hydralazine | Direct Arterial Vasodilator | 0.5-2 mg/kg PO q12h | Effective in dogs; used for refractory cases; can cause reflex tachycardia |
| Benazepril | ACE Inhibitor | 0.25-0.5 mg/kg PO q12-24h | Mild BP reduction; useful for proteinuria; hepatic metabolism |
| Enalapril | ACE Inhibitor | 0.25-0.5 mg/kg PO q12-24h | Similar to benazepril; renal excretion |
| Telmisartan | ARB (Angiotensin Receptor Blocker) | 1 mg/kg PO q24h | Effective for refractory hypertension; often combined with amlodipine |
| Prazosin | Alpha-1 Blocker | 0.5-2 mg/dog PO q8-12h | Mixed vasodilator; tolerance develops; rarely used as primary agent |
Board Tip: In dogs, AMLODIPINE and HYDRALAZINE are the only consistently effective antihypertensive drugs for lowering blood pressure. ACE inhibitors (benazepril, enalapril) alone are generally NOT potent enough to control severe hypertension but are useful for reducing proteinuria and may be combined with amlodipine.
Treatment Algorithm
- Step 1: Start amlodipine at 0.1-0.2 mg/kg PO q24h
- Step 2: Recheck BP in 7-10 days
- Step 3: If BP still elevated, increase amlodipine to maximum (0.5 mg/kg q12h) OR add second agent
- Step 4: Consider adding telmisartan (1 mg/kg q24h) or hydralazine for refractory cases
- Step 5: If proteinuria present, add ACE inhibitor or ARB
- Step 6: Once controlled, monitor BP every 3-6 months
Hypertensive Emergency Management
A hypertensive emergency occurs when SBP exceeds 200 mm Hg with acute, progressive target organ damage. This requires immediate intervention:
- Amlodipine 0.2-0.5 mg/kg PO as first-line oral therapy
- Hydralazine 0.1-0.25 mg/kg IV bolus for rapid reduction (with caution)
- Continuous BP monitoring during treatment
- Avoid precipitous drops in BP (risk of cerebral or renal ischemia)
- Target 25% reduction in SBP over first 1-2 hours, then gradual normalization
Monitoring and Long-Term Management
- Initial stabilization: Recheck BP every 1-3 days until controlled
- Stable patients: Monitor BP every 3-6 months
- Target BP: SBP less than 160 mm Hg (ideally less than 140 mm Hg)
- Lab monitoring: Renal values, UPC ratio, electrolytes periodically
- Ophthalmic exams: Fundic examination to monitor for resolution or progression of retinopathy
- Treat underlying cause: Address CKD, Cushing's disease, etc. when possible
Prognosis
Prognosis depends on the underlying cause and severity of target organ damage at diagnosis. With appropriate treatment, blood pressure can often be controlled. However, lifelong therapy and monitoring are typically required. Vision may be recovered in some patients with prompt treatment of hypertensive retinopathy, though permanent blindness is common with complete retinal detachment. Proteinuria severity and renal function decline are associated with shorter survival times in hypertensive dogs with CKD.
Practice Question
| A 10-year-old female spayed Miniature Schnauzer is presented for acute onset bilateral blindness noticed this morning. The owner reports the dog has been drinking more water over the past few months. Physical examination reveals mydriatic pupils with absent pupillary light reflexes bilaterally. Fundoscopic examination shows bilateral retinal detachments with subretinal hemorrhage. The dog's body condition score is 7/9. Blood pressure measured using Doppler ultrasonography at the forelimb reveals a systolic blood pressure of 220 mm Hg. Which of the following is the MOST appropriate initial treatment for this patient? A. Enalapril 0.5 mg/kg PO q12h B. Amlodipine 0.2 mg/kg PO q24h C. Phenylephrine eye drops for pupil dilation D. Furosemide 2 mg/kg IV E. Prednisone 1 mg/kg PO q12h for optic neuritis |
|---|
Correct Answer: B
Explanation
Amlodipine (Option B) is the correct answer. This patient is presenting with a hypertensive emergency with acute target organ damage (bilateral retinal detachment causing blindness). The SBP of 220 mm Hg is severely elevated and requires immediate intervention. Amlodipine is a calcium channel blocker and potent arterial vasodilator that is the first-line treatment for systemic hypertension in dogs. Given the history of polyuria/polydipsia in an older, overweight Miniature Schnauzer, underlying conditions such as CKD, hyperadrenocorticism, or diabetes mellitus should be investigated as causes of secondary hypertension.
Option A (Enalapril) is incorrect. While ACE inhibitors have a role in managing proteinuria and may be part of long-term management, they are not potent enough as monotherapy to adequately reduce severely elevated blood pressure in dogs. ACE inhibitors alone typically produce only mild reductions in BP.
Option C (Phenylephrine) is incorrect. Phenylephrine is an alpha-adrenergic agonist that causes vasoconstriction and would worsen hypertension. It would be contraindicated in this case. Additionally, dilating the pupils would not address the underlying retinal pathology.
Option D (Furosemide) is incorrect. While diuretics may have some role in volume-mediated hypertension, they are not effective as primary antihypertensive therapy in dogs. Furosemide would not adequately address this severe arterial hypertension.
Option E (Prednisone) is incorrect. This is not optic neuritis—it is hypertensive retinopathy with retinal detachment. Glucocorticoids would not address the underlying hypertension and could potentially worsen it (as corticosteroids can elevate blood pressure through sodium retention and other mechanisms).
High-Yield Note: When you see an older dog with acute bilateral blindness, retinal detachment, and severe hypertension, think SECONDARY HYPERTENSION. Always look for PU/PD and other signs pointing to CKD, Cushing's disease, or diabetes mellitus. Amlodipine is the first-line treatment, and prompt therapy may allow visual recovery if initiated before permanent retinal damage occurs.
Summary: Key Takeaways
- Definition: SBP greater than or equal to 160 mm Hg = hypertensive; greater than or equal to 180 mm Hg = severely hypertensive
- Etiology: Secondary hypertension predominates (CKD, Cushing's, DM, pheochromocytoma)
- Target organs: Eyes, kidneys, heart, brain—look for TOD on exam
- Diagnosis: Doppler or oscillometry; proper technique and cuff size critical
- Treatment: Amlodipine is first-line in dogs; ACE inhibitors alone are insufficient
- Monitoring: Target SBP less than 160 mm Hg; recheck BP every 3-6 months when stable
- Prognosis: Depends on underlying cause and severity of TOD; lifelong management usually required
Memory Tip: "HYPER Dogs"
H = Heart damage (LVH, murmurs) Y = You must measure BP (correct technique!) P = Proteinuria and renal damage E = Eyes (retinopathy, blindness) R = Rx = Amlodipine first-line!
Image Sources
- ACVIM Blood Pressure Classification Chart - Adapted from: Acierno MJ, et al. ACVIM consensus statement: Guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats. J Vet Intern Med. 2018;32:1803-1822. (Open Access CC BY-NC 4.0) URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC6271319/ - See Table 4 and Figure 1
- Hypertensive Retinopathy Image - Beckwith-Cohen B, Petersen-Jones SM. Manifestations of systemic disease in the retina and fundus of cats and dogs. Front Vet Sci. 2024;11:1337062. (Open Access CC BY 4.0) URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC10912207/ - See Figure 11 (Retinal hemorrhages)
- Echocardiogram showing LVH - From veterinary cardiology educational resources, consider using images from Merck Veterinary Manual (free access). URL: https://www.merckvetmanual.com/circulatory-system/various-cardiovascular-diseases-in-dogs-and-cats/systemic-and-pulmonary-hypertension-in-dogs-and-cats
- Doppler Blood Pressure Measurement Technique - Today's Veterinary Practice. Blood Pressure Monitoring From a Nursing Perspective, Part 2. (Educational resource) URL: https://todaysveterinarypractice.com/cardiology/todays-technician-blood-pressure-monitoring-from-a-nursing-perspective-part-2-blood-pressure-monitoring-techniques/ - See Figures 1-2
References
- Acierno MJ, Brown S, Coleman AE, et al. ACVIM consensus statement: Guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats. J Vet Intern Med. 2018;32(6):1803-1822.
- Brown S, Atkins C, Bagley R, et al. Guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats. J Vet Intern Med. 2007;21(3):542-558.
- LeBlanc NL, Stepien RL, Bentley E. Ocular lesions associated with systemic hypertension in dogs: 65 cases (2005-2007). J Am Vet Med Assoc. 2011;238(7):915-921.
- Cole LP, Jepson R, Humm K. Hypertension, retinopathy, and acute kidney injury in dogs: A prospective study. J Vet Intern Med. 2020;34(5):1940-1947.
- Caro-Vadillo A, Daza-González MA, Gonzalez-Alonso-Alegre E, et al. Effect of a combination of telmisartan and amlodipine in hypertensive dogs. Vet Rec Case Rep. 2018;6:e000471.
- Beckwith-Cohen B, Petersen-Jones SM. Manifestations of systemic disease in the retina and fundus of cats and dogs. Front Vet Sci. 2024;11:1337062.
- Fowler BL, Stefanovski D, Hess RS, McGonigle K. Effect of telmisartan, angiotensin-converting enzyme inhibition, or both on proteinuria and blood pressure in dogs. J Vet Intern Med. 2021;35(3):1231-1237.
- Merck Veterinary Manual. Systemic and Pulmonary Hypertension in Dogs and Cats. Available at: https://www.merckvetmanual.com
Practice NAVLE Questions
Test your knowledge with 10,000+ exam-style questions, detailed explanations, and timed exams.
Start Your Free Trial →