Canine Systemic Hypertension Navle Study Guide
Canine Systemic Hypertension
NAVLE Study Guide
Cardiovascular System | Species: Canine
Estimated Read Time: 30-35 minutes | Last Updated: December 2024
Overview and Clinical Importance
Systemic hypertension refers to sustained elevations in systemic arterial blood pressure. In dogs, systolic blood pressure consistently greater than 140 mmHg or diastolic pressure greater than 90 mmHg is considered elevated. However, the ACVIM Consensus Guidelines recommend that treatment be initiated when systolic pressure persistently exceeds 160 mmHg, as this level is associated with moderate-to-high risk for target organ damage (TOD).
Unlike in cats where hypertension is commonly recognized, canine hypertension has historically been underdiagnosed. However, it is a clinically significant condition that can cause serious complications affecting the eyes, kidneys, heart, and brain. Understanding the diagnosis, underlying causes, and treatment of canine hypertension is essential for NAVLE success.
High-Yield Note: In dogs, hypertension is almost always SECONDARY to an underlying disease. Primary (essential/idiopathic) hypertension is rare in dogs, unlike in humans. Always search for an underlying cause!
Learning Objectives
- Classify systemic hypertension by ACVIM blood pressure categories and associated risk of target organ damage
- Identify common underlying diseases causing secondary hypertension in dogs
- Demonstrate proper blood pressure measurement technique (Doppler and oscillometric)
- Recognize clinical signs of target organ damage, particularly hypertensive retinopathy
- Select appropriate antihypertensive therapy for canine patients
Blood Pressure Classification
The ACVIM Consensus Guidelines (2018) classify blood pressure based on the risk of developing target organ damage (TOD). Treatment decisions should consider both the blood pressure level and the presence or absence of TOD.
Table 1: ACVIM Blood Pressure Classification Chart or Blood Pressure Measurement on Dog
| Category | Systolic BP (mmHg) | Risk of TOD | Action |
|---|---|---|---|
| Normotensive | Less than 140 | Minimal | Routine monitoring |
| Pre-hypertensive | 140-159 | Low | Monitor every 3-6 months |
| Hypertensive | 160-179 | Moderate | Confirm over 1-2 weeks; treat if persistent |
| Severely Hypertensive | 180 or greater | High | Immediate treatment recommended |
Board Tip: Remember the magic number: 160 mmHg systolic. This is the threshold at which treatment should be considered in dogs with persistent elevation. If TOD is present, treat immediately regardless of the number of measurements.
Etiology of Canine Hypertension
Canine hypertension is classified as either primary (idiopathic/essential) or secondary. Secondary hypertension, which accounts for the vast majority of cases in dogs, occurs due to an identifiable underlying disease.
Common Causes of Secondary Hypertension
| Underlying Disease | Prevalence of HTN | Mechanism |
|---|---|---|
| Chronic Kidney Disease (CKD) | 30-93% | RAAS activation, sodium retention, reduced vasodilators |
| Hyperadrenocorticism (Cushing's) | 59-86% | Cortisol increases vascular tone, sodium retention, RAAS activation |
| Pheochromocytoma | ~50% | Catecholamine excess causes vasoconstriction, tachycardia |
| Diabetes Mellitus | 24-46% | Vascular dysfunction, often concurrent CKD |
| Primary Hyperaldosteronism | Common | Aldosterone causes sodium and water retention |
| Obesity | Variable | Increased cardiac output, RAAS activation, insulin resistance |
Memory Aid: "CHOP DOG"
Causes of Canine Hypertension:
- C - Chronic Kidney Disease (most common)
- H - Hyperadrenocorticism (Cushing's disease)
- O - Obesity
- P - Pheochromocytoma
- D - Diabetes mellitus
- O - Other endocrine (hypothyroidism - uncommon)
- G - Glomerular disease (protein-losing nephropathy)
Blood Pressure Measurement Technique
You should know how a Doppler Blood Pressure Measurement device looks like…
Accurate blood pressure measurement is critical for diagnosis. The ACVIM recommends following a standardized protocol to minimize situational (white coat) hypertension, which can cause falsely elevated readings due to stress.
Standardized Measurement Protocol
- Allow the patient 5-10 minutes to acclimate to the environment
- Measure BP in a quiet, isolated area away from other animals
- Have the owner present if possible to reduce anxiety
- Position patient in lateral or sternal recumbency
- Place the cuff at heart level (right atrium)
- Select proper cuff size: width = 40% of limb circumference in dogs
- Discard first measurement; obtain 5-7 consecutive readings
- Average the readings for final BP value
High-Yield Note: Cuff size is CRITICAL! A cuff too small will give FALSELY HIGH readings. A cuff too large will give FALSELY LOW readings. The cuff width should be 40% of the limb circumference in dogs (30-40% in cats).
Doppler vs. Oscillometric Methods
| Feature | Doppler | Oscillometric |
|---|---|---|
| Measures | Systolic BP (most reliable) | Systolic, MAP, Diastolic |
| Best Used In | Small dogs, cats, hypotensive patients | Medium-large dogs, automated monitoring |
| Advantages | Works in low flow states, more accurate in small patients | Automated, provides MAP (most reliable value) |
| Limitations | Manual, no diastolic/MAP, technique-dependent | Less reliable with movement, arrhythmias, small patients |
| Cuff Placement | Proximal to probe on limb or tail | Proximal limb or tail base |
Target Organ Damage (TOD)
Sustained hypertension can cause damage to organs with rich arteriolar blood supply. The eyes, kidneys, heart, and brain are most commonly affected. Recognizing TOD is critical because its presence indicates immediate treatment is needed, regardless of how many times BP has been measured.
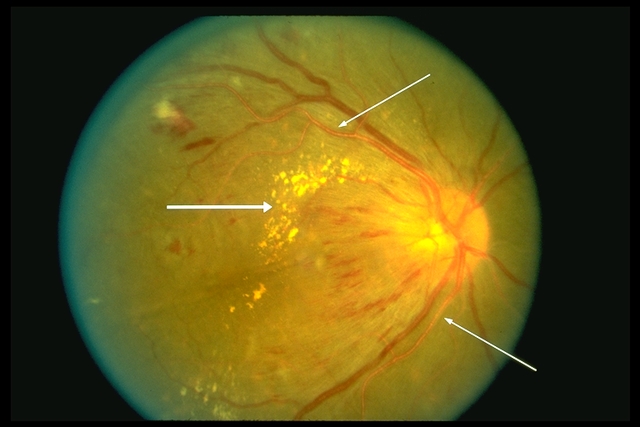
Figure 1: Hypertensive Retinopathy showing Retinal Hemorrhage or Detachment
Ocular (Hypertensive Retinopathy)
Ocular lesions are present in approximately 62% of hypertensive dogs. Visual disturbance or acute blindness is often the presenting complaint.
- Retinal hemorrhages - flame-shaped, punctate, or preretinal
- Retinal detachment - serous, can cause acute blindness
- Hyphema - blood in anterior chamber
- Tortuous retinal vessels - "box-carring" appearance
- Subretinal edema - fluid accumulation
- Papilledema - optic nerve swelling
- Secondary glaucoma
Renal
- Progressive glomerular damage and glomerulosclerosis
- Proteinuria (elevated UPC ratio)
- Progression of chronic kidney disease
Cardiac
- Left ventricular hypertrophy (concentric)
- Diastolic dysfunction
- Systolic murmur may develop
Neurologic (Hypertensive Encephalopathy)
- Acute onset seizures
- Altered mentation, disorientation
- Ataxia, head tilt, vestibular signs
- Cerebrovascular accident (stroke)
Board Tip: When a dog presents with acute blindness, bilateral mydriasis, and absent PLRs, ALWAYS check blood pressure! Hypertensive retinopathy with retinal detachment is a common cause. Early treatment (within 3 weeks of onset) offers the best chance of visual recovery.
Antihypertensive Treatment
Treatment goals include: reducing BP to less than 160 mmHg (ideally less than 140 mmHg), preventing TOD, and treating the underlying cause. In dogs, ACE inhibitors are first-line therapy. Amlodipine is added for refractory cases. This differs from cats, where amlodipine is first-line.
RAAS System Mechanism of ACE Inhibitors
- Low Blood Pressure/Volume → Kidneys release Renin.
- Renin acts on liver's Angiotensinogen → Angiotensin I (Ang I).
- Ang I passes through lungs → ACE converts it to Angiotensin II (Ang II).
- Ang II Effects:
- Vasoconstriction (narrows vessels).
- Stimulates Adrenal Glands to release Aldosterone (kidneys retain Na+/Water, excrete K+).
- Stimulates Pituitary to release ADH (kidneys retain Water).
- Increases thirst.
- Result: Increased blood volume & vasoconstriction → ↑ Blood Pressure
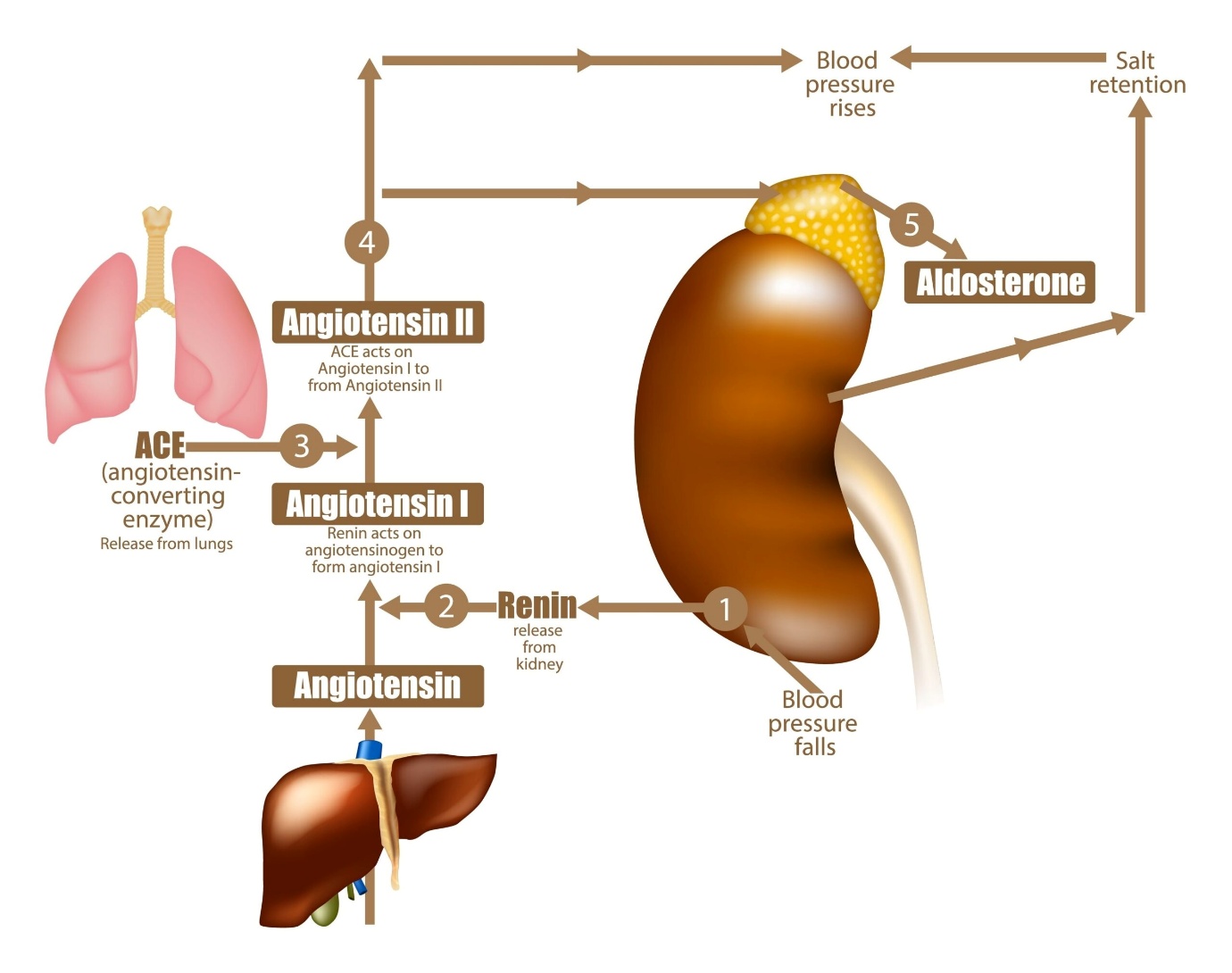
Figure 2: RAAS mechanism.
Antihypertensive Drug Summary
| Drug Class | Drug | Dose (Dog) | Mechanism | Key Points |
|---|---|---|---|---|
| ACE Inhibitor | Enalapril Benazepril | 0.5 mg/kg PO q12-24h | Block angiotensin II formation; vasodilation | First-line in dogs; monitor renal values; antiproteinuric |
| Ca Channel Blocker | Amlodipine | 0.1-0.5 mg/kg PO q24h | Block L-type Ca channels; arteriolar dilation | Add if ACEi insufficient; potent vasodilator; combine with ACEi |
| ARB | Telmisartan | 1 mg/kg PO q24h | Block AT1 receptor; vasodilation | Alternative/addition to ACEi; good for refractory cases |
| Direct Vasodilator | Hydralazine | 0.5-2 mg/kg PO q12h | Direct arteriolar smooth muscle relaxation | Hypertensive crisis; reflex tachycardia common |
| Alpha Blocker | Phenoxybenzamine | 0.25-0.5 mg/kg PO q12h | Block alpha-1 receptors; vasodilation | Pheochromocytoma (start 2 weeks pre-surgery) |
Treatment Algorithm for Dogs
- First-line: ACE inhibitor (enalapril or benazepril 0.5 mg/kg PO q12-24h)
- If inadequate after 1-2 weeks: Add amlodipine (0.1-0.25 mg/kg PO q24h)
- If still inadequate: Increase amlodipine to 0.5 mg/kg or add telmisartan
- Hypertensive crisis (greater than 200 mmHg with TOD): Consider hydralazine or IV therapy
- Pheochromocytoma: Phenoxybenzamine first, then add beta-blocker if needed (never beta-blocker alone!)
High-Yield Note: For pheochromocytoma, ALWAYS start alpha-blockade (phenoxybenzamine) BEFORE beta-blockade. Starting a beta-blocker alone causes unopposed alpha stimulation leading to severe hypertensive crisis. Alpha-blockade should be initiated 2 weeks before adrenalectomy.
Memory Aid: "Dogs ACE it, Cats AMLify"
Dogs: ACE inhibitor first-line (enalapril, benazepril) | Cats: AMLodipine first-line
Monitoring and Follow-up
- Recheck BP: 7-10 days after starting/changing therapy
- Stable patients: Every 1-4 months depending on severity
- Monitor renal values: 5-7 days after starting ACEi/ARB (may see mild creatinine increase)
- Target BP: Less than 160 mmHg (ideally less than 140 mmHg)
- Watch for hypotension: Weakness, lethargy if BP drops below 120 mmHg
- Fundic examination: Regular monitoring for ocular TOD resolution
Practice Question
| A 10-year-old female spayed Miniature Schnauzer presents with acute onset blindness that the owner first noticed this morning. On examination, bilateral mydriasis with absent pupillary light reflexes is noted. Fundic examination reveals bilateral bullous retinal detachments with multifocal retinal hemorrhages. The dog's body condition is normal, and no other abnormalities are detected on physical examination. Doppler blood pressure measurement reveals a systolic pressure of 245 mmHg. Which of the following is the most appropriate initial diagnostic workup to identify the underlying cause of this dog's hypertension? A. Thoracic radiographs and echocardiogram B. Complete blood count, serum chemistry panel, urinalysis with UPC ratio C. Low-dose dexamethasone suppression test only D. Abdominal ultrasound only E. MRI of the brain |
|---|
Correct Answer: B
Explanation
Option B (CBC, chemistry, urinalysis with UPC ratio) is correct because canine hypertension is almost always secondary to an underlying disease. The initial diagnostic workup should screen for the most common causes: chronic kidney disease (most common), hyperadrenocorticism (Cushing's disease), diabetes mellitus, and protein-losing nephropathy. A complete blood count, serum chemistry panel (including BUN, creatinine, glucose, liver enzymes, electrolytes), and urinalysis with urine protein-to-creatinine ratio will help identify renal disease, diabetes, and proteinuria. This is the appropriate starting point before pursuing more specific testing.
Option A (thoracic radiographs and echocardiogram) is incorrect because while cardiac evaluation may eventually be warranted to assess for left ventricular hypertrophy (a consequence of hypertension), cardiac disease is rarely the primary cause of hypertension in dogs. Primary cardiac causes of hypertension are uncommon.
Option C (LDDS test only) is incorrect because while hyperadrenocorticism is a common cause of hypertension, testing for Cushing's disease should not be performed in isolation. A broader initial workup is needed to screen for all common causes, especially CKD, which is the most common cause.
Option D (abdominal ultrasound only) is incorrect because while ultrasound can identify structural abnormalities (adrenal masses, kidney changes), it does not provide the functional information obtained from bloodwork and urinalysis that is critical for diagnosing CKD, diabetes, or determining the degree of proteinuria.
Option E (brain MRI) is incorrect because the neurologic signs (blindness) in this case are due to hypertensive retinopathy causing retinal detachment, not primary brain disease. The brain is not the underlying cause of the hypertension.
Board Tip: This case demonstrates several high-yield concepts: (1) Acute blindness with bilateral mydriasis and retinal detachment should prompt immediate BP measurement; (2) Hypertension in dogs is almost always secondary - search for the cause; (3) CKD is the most common underlying cause, followed by Cushing's disease; (4) The Miniature Schnauzer is predisposed to both Cushing's disease and hyperlipidemia, but initial workup should still be comprehensive.
Key Takeaways
- Threshold for treatment: Systolic BP persistently greater than 160 mmHg OR any BP with TOD present
- Etiology in dogs: Almost always secondary (CKD most common, then Cushing's, pheochromocytoma, diabetes)
- Cuff size: 40% of limb circumference - too small = false HIGH, too large = false LOW
- Target organs: Eyes (retinopathy most common), kidneys, heart (LVH), brain
- First-line therapy in dogs: ACE inhibitor (enalapril, benazepril); add amlodipine if refractory
- Pheochromocytoma: Alpha-blockade (phenoxybenzamine) BEFORE beta-blockade; never beta-blocker alone
- Monitoring: Recheck BP in 7-10 days; monitor renal values with ACEi/ARB therapy
- Visual prognosis: Best if treated within 3 weeks of onset; retinal detachment may resolve with BP control
Image Sources/Credits
1. https://eyewiki.org/File:Malignant_HTN_RET.jpg
2. https://phlebotomycareertraining.com/renin-angiotensin-pathway-explained-in-under-a-minute/
3. PMC Open Access - Ocular Lesions Associated with Systemic Hypertension in Dogs
URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC4187359/
4. Frontiers in Veterinary Science - Manifestations of Systemic Disease in the Retina (Open Access)
URL: https://www.frontiersin.org/journals/veterinary-science/articles/10.3389/fvets.2024.1337062/full
5. Clinician's Brief - Top 5 Ocular Consequences of Systemic Hypertension
URL: https://www.cliniciansbrief.com/article/top-5-ocular-consequences-systemic-hypertension
6. WikiVet - Blood Pressure Measurement (Educational, Free Use)
URL: https://en.wikivet.net/Blood_Pressure_Measurement
References
1. Acierno MJ, Brown S, Coleman AE, et al. ACVIM consensus statement: Guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats. J Vet Intern Med. 2018;32(6):1803-1822.
2. Brown S, Atkins C, Bagley R, et al. Guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats. J Vet Intern Med. 2007;21(3):542-558.
3. Cole LP, Jepson R, Dawson C, Humm K. Hypertension, retinopathy, and acute kidney injury in dogs: A prospective study. J Vet Intern Med. 2020;34:1940-1947.
4. Cortadellas O, del Palacio MJF, Talavera J, Bayón A. Systemic hypertension in dogs with leishmaniasis: Prevalence and clinical consequences. J Vet Intern Med. 2006;20(4):941-947.
5. LeBlanc NL, Stepien RL, Bentley E. Ocular lesions associated with systemic hypertension in dogs: 65 cases (2005-2007). J Am Vet Med Assoc. 2011;238(7):915-921.
6. Smets P, Meyer E, Maddens B, Duchateau L, Daminet S. Cushing's syndrome, glucocorticoids and the kidney. Gen Comp Endocrinol. 2010;169(1):1-10.
7. Herrera MA, Mehl ML, Kass PH, et al. Predictive factors and the effect of phenoxybenzamine on outcome in dogs undergoing adrenalectomy for pheochromocytoma. J Vet Intern Med. 2008;22(6):1333-1339.
8. Grauer GF. Treatment of systemic hypertension in dogs and cats. In: Bonagura JD, Twedt DC, eds. Kirk's Current Veterinary Therapy XV. Elsevier; 2014:713-717.
9. Reusch CE, Schellenberg S, Wenger M. Endocrine hypertension in small animals. Vet Clin North Am Small Anim Pract. 2010;40(2):335-352.
10. Caro-Vadillo A, Daza-González MA, Gonzalez-Alonso-Alegre E, et al. Effect of a combination of telmisartan and amlodipine in hypertensive dogs. Vet Rec Case Rep. 2018;6:e000471.
Practice NAVLE Questions
Test your knowledge with 10,000+ exam-style questions, detailed explanations, and timed exams.
Start Your Free Trial →