Canine Pericardial Disease Study Guide
Canine Pericardial Disease
NAVLE Study Guide
Cardiovascular System | Species: Canine
Estimated Read Time: 30-35 minutes | Last Updated: December 2024
Overview and Clinical Importance
Pericardial disease in dogs encompasses a range of conditions affecting the pericardium, the fibroserous membrane surrounding the heart. While pericardial diseases account for approximately 5% of all cardiovascular disorders in dogs, they represent a critically important cause of right-sided heart failure and can present as life-threatening emergencies. Pericardial effusion is by far the most common manifestation, accounting for greater than 90% of all pericardial disorders in dogs.
Understanding the etiology, pathophysiology, diagnosis, and management of pericardial disease is essential for the NAVLE, as it is frequently tested and requires integration of knowledge across cardiovascular physiology, diagnostics, and emergency medicine.
Learning Objectives
- Differentiate between the etiologies of pericardial effusion including neoplastic, idiopathic, and congenital causes
- Recognize the clinical signs and physical examination findings of cardiac tamponade
- Interpret diagnostic findings including radiography, ECG, and echocardiography in pericardial disease
- Describe the technique and indications for pericardiocentesis
- Apply appropriate treatment strategies based on the underlying cause and understand prognosis
Pericardial Anatomy and Physiology
The pericardium is a fibroserous sac consisting of two layers: the visceral pericardium (epicardium) which is closely adherent to the heart surface, and the parietal pericardium which is the outer fibrous layer. The pericardial space between these layers normally contains 2-10 mL of clear, serous fluid that serves as a lubricant.
Functions of the pericardium include: anchoring the heart within the mediastinum, limiting excessive cardiac motion, providing a barrier against infection, and maintaining the pressure-volume relationship during rapid changes in cardiac filling.
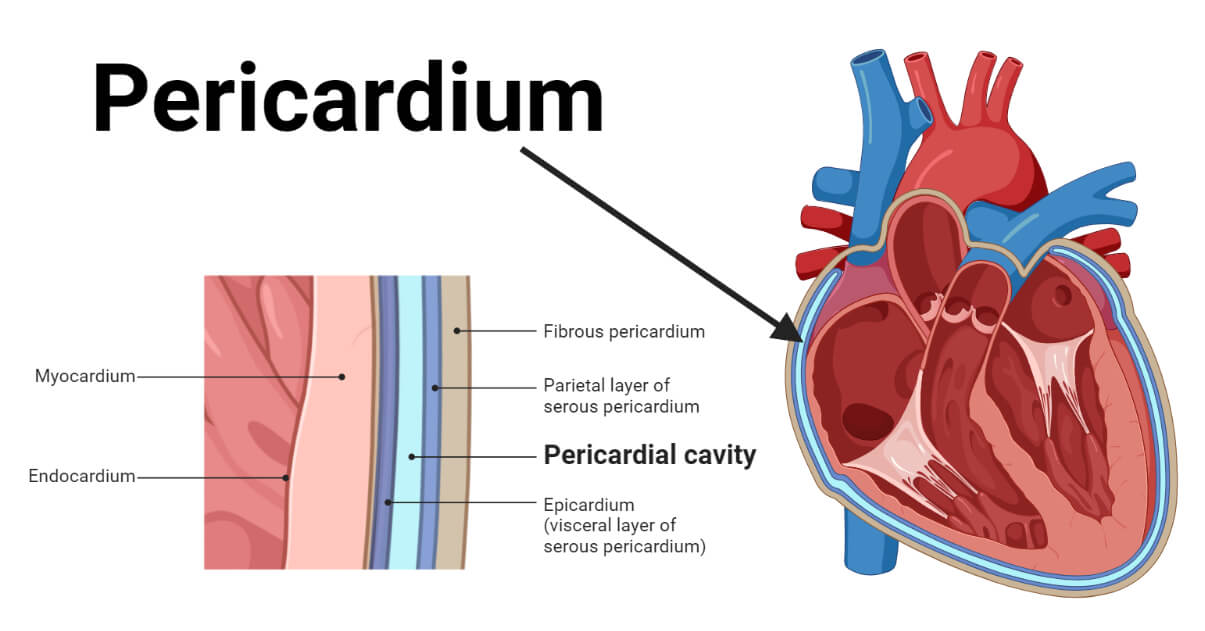
Figure 1 - Diagram of normal pericardial anatomy showing the visceral and parietal layers, pericardial space, and relationship to cardiac structures
High-Yield Note: The pericardium's ability to stretch is time-dependent. Rapid fluid accumulation (as little as 25-100 mL) can cause tamponade, while chronic, slow accumulation may allow up to 2 liters before clinical signs develop. This concept explains why acute hemorrhage is often more immediately life-threatening than chronic effusions.
Etiology of Pericardial Disease
Causes of Pericardial Effusion
| Category | Specific Causes |
|---|---|
| Neoplastic (50-70%) | Hemangiosarcoma: Most common (34%); typically right atrial/auricular; Golden Retrievers, German Shepherds predisposed Heart Base Tumors: Chemodectoma/aortic body tumor (8%); Boxers, Boston Terriers, Bulldogs predisposed Mesothelioma: (14%); difficult to diagnose; diffuse pericardial involvement Other: Ectopic thyroid carcinoma, lymphoma, metastatic carcinoma |
| Idiopathic (20-30%) | Benign pericardial effusion; typically hemorrhagic Male, middle-aged, large-breed dogs (Golden Retrievers, German Shepherds, Great Danes, Saint Bernards) May recur; subtotal pericardiectomy often curative |
| Congenital | Peritoneopericardial diaphragmatic hernia (PPDH): Most common congenital defect; Weimaraners predisposed Pericardial cysts: Rare; usually asymptomatic |
| Infectious | Bacterial: Actinomyces, Nocardia (often from migrating grass awns/foxtails) Fungal: Coccidioides immitis (endemic regions) |
| Other Causes | Left atrial rupture (secondary to severe mitral valve disease) Trauma Anticoagulant rodenticide toxicosis Congestive heart failure (typically small volume) Uremia, hypoalbuminemia |
Board Tip: Remember breed predispositions with "G.G.B.B." - Golden retrievers and German shepherds = Hemangiosarcoma; Boxers, Boston terriers, and Bulldogs (Brachycephalics) = Heart base tumors (chemodectoma). This is a high-yield NAVLE association!
Pathophysiology of Cardiac Tamponade
Cardiac tamponade occurs when intrapericardial pressure rises high enough to impair cardiac filling. The pericardium has a steep pressure-volume relationship once its compliance limit is exceeded.
Hemodynamic Consequences
- Increased intrapericardial pressure exceeds right atrial diastolic pressure (normally 5 mmHg)
- Right heart compression occurs first due to lower pressures (right-sided signs predominate)
- Decreased venous return leads to reduced preload and stroke volume
- Reduced cardiac output triggers compensatory mechanisms (tachycardia, vasoconstriction)
- Cardiogenic shock develops if untreated
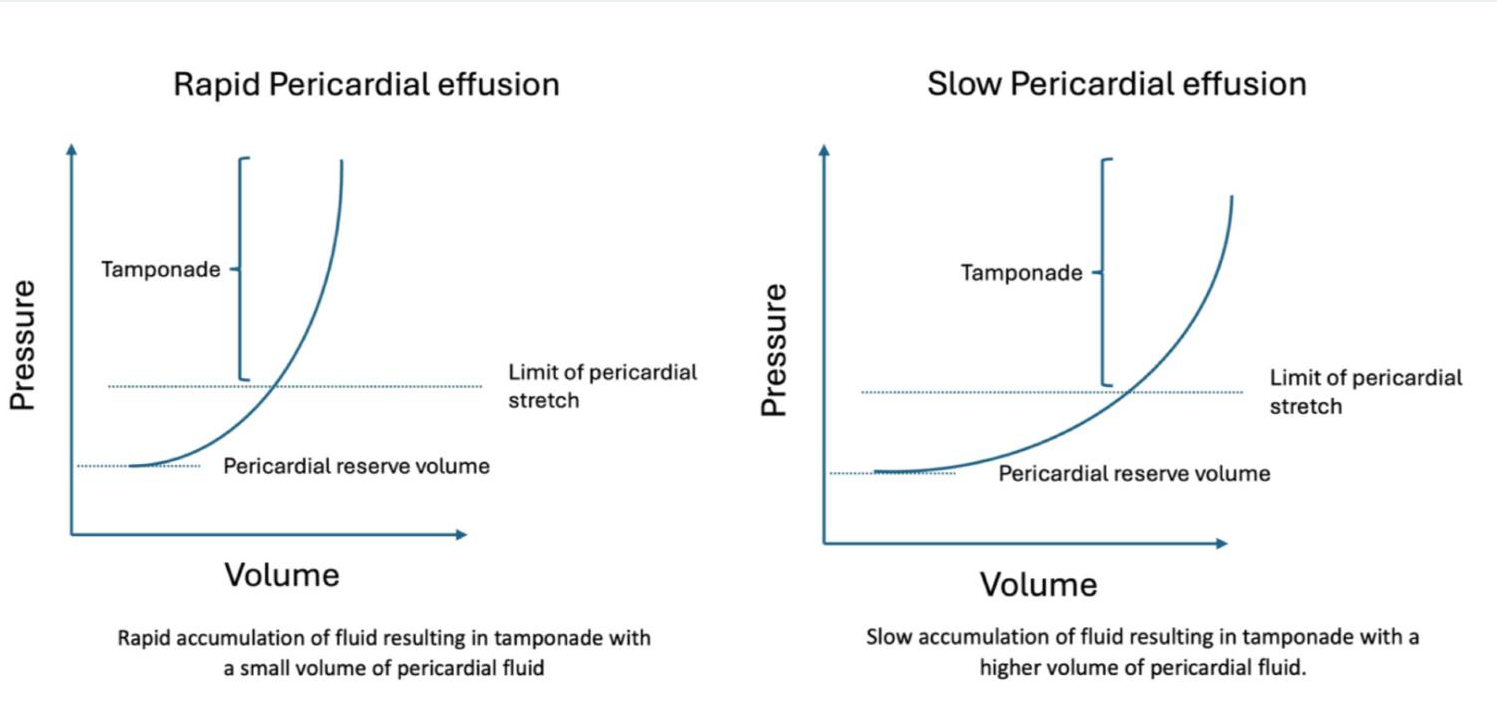
Figure 2 - Pressure-volume curve demonstrating the relationship between pericardial fluid volume and intrapericardial pressure, showing the steep J-shaped curve once compliance is exceeded
High-Yield Note: Right-sided pressures only need to increase from 5 mmHg to 10-15 mmHg to cause signs of heart failure, while left-sided pressures must exceed 20 mmHg. This explains why right-sided heart failure (ascites, jugular distension) predominates in cardiac tamponade rather than left-sided signs (pulmonary edema).
Clinical Presentation
Signalment and History
Pericardial effusion most commonly affects middle-aged to older (mean age 6-9 years), large-breed, male dogs. Common presenting complaints include:
- Lethargy and weakness (most common)
- Exercise intolerance
- Collapse or syncope
- Abdominal distension (ascites)
- Anorexia
- Dyspnea or tachypnea
- Cough (less common)
Physical Examination Findings
Beck's Triad - The classic triad of cardiac tamponade:
- Muffled/distant heart sounds (most consistent finding)
- Jugular venous distension
- Systemic hypotension (weak/absent femoral pulses)
| Finding | Clinical Significance |
|---|---|
| Muffled heart sounds | Most consistent finding; fluid insulates heart sounds |
| Pulsus paradoxus | Exaggerated decrease in pulse strength during inspiration; greater than 10 mmHg systolic pressure variation |
| Tachycardia | Compensatory response to decreased cardiac output |
| Hepatojugular reflux | Positive test indicates elevated central venous pressure |
| Ascites | Result of chronic right-sided heart failure; most common clinical sign |
| Hepatomegaly | Passive congestion from elevated venous pressure |
Memory Tip: "MUFFLED HEARTS" - Muffled sounds, Undetectable pulse (weak), Fluid (ascites), Falling blood pressure, Lethargy, Elevated jugular veins, Distended abdomen, Heart rate increased (tachycardia), Exercise intolerance, Acute collapse, Right-sided failure signs, Tamponade, Syncope
Diagnostic Evaluation
Thoracic Radiography
Radiographic findings depend on the volume and chronicity of the effusion:
- Globoid cardiac silhouette: Classic "basketball" or "pumpkin" shape with sharp, well-defined borders
- Increased vertebral heart score (VHS): Greater than or equal to 10.7 is suggestive
- Dilated caudal vena cava: Indicates elevated right-sided pressures
- Heart base bulge: May be visible with heart base tumors
- Pleural effusion: May be concurrent, especially with mesothelioma
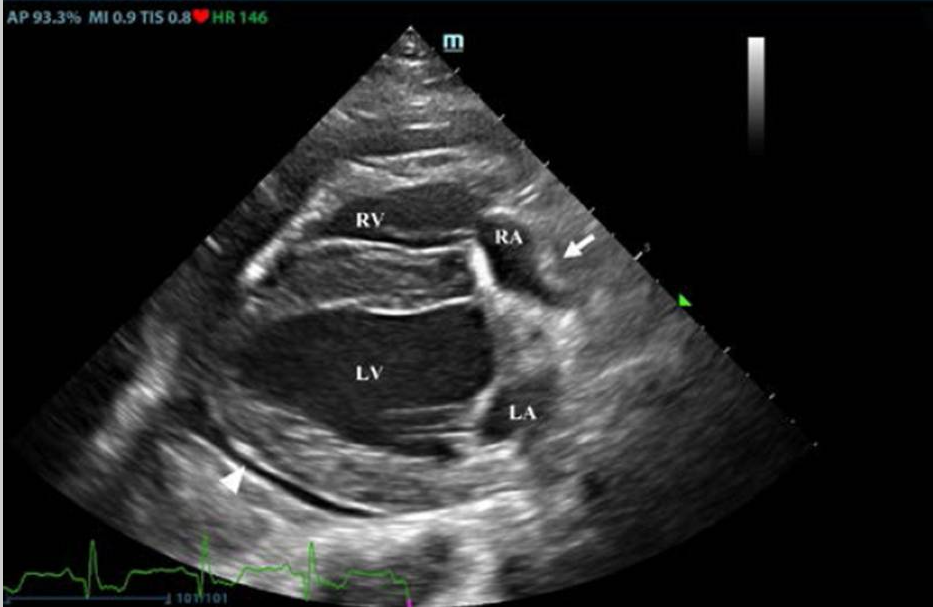
Figure 3 - Lateral and VD thoracic radiographs demonstrating classic globoid cardiac silhouette with sharp margins and dilated caudal vena cava in a dog with pericardial effusion
High-Yield Note: Radiographs may be NORMAL in acute pericardial effusion because the pericardium has not had time to stretch! Never rule out pericardial disease based on radiographs alone. If clinical suspicion is high, proceed with echocardiography. Also, avoid VD positioning in unstable patients - use DV instead.
Electrocardiography (ECG)
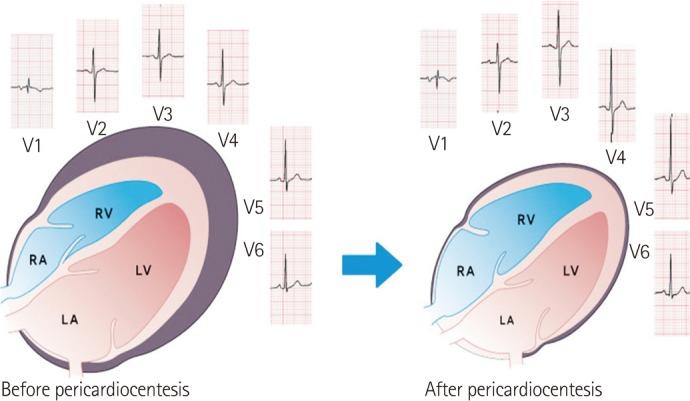
Figure 4 – Before and after pericardiocentesis
| ECG Finding | Description and Significance |
|---|---|
| Sinus tachycardia | Most common finding; compensatory response |
| Low-voltage QRS complexes | R wave less than 1.0 mV in lead II; fluid insulates electrical signal |
| Electrical alternans | Alternating QRS amplitude (tall-short-tall pattern); heart "swinging" in fluid; PATHOGNOMONIC for large effusion but not always present |
| ST segment changes | May indicate myocardial hypoxia or epicardial injury |
| Ventricular arrhythmias | May occur with neoplastic causes (especially hemangiosarcoma) |
Echocardiography
Echocardiography is the GOLD STANDARD for diagnosing pericardial effusion. Point-of-care ultrasound (POCUS) using the TFAST protocol and the diaphragmatico-hepatic (DH) view is highly sensitive and can be performed rapidly in emergency settings.
Key Echocardiographic Findings
- Anechoic/hypoechoic space: Echo-free space between pericardium and epicardium
- Cardiac swinging: Heart moves back and forth within fluid
- Right atrial collapse: During diastole; indicates tamponade physiology
- Right ventricular collapse: In early diastole; more severe tamponade
- Cardiac masses: Right atrial (hemangiosarcoma) or heart base (chemodectoma)
- Dilated hepatic veins and caudal vena cava: Indicates elevated right-sided pressures
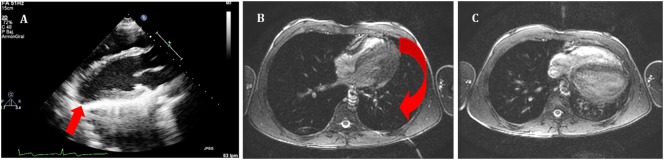
Figure 5 - Right parasternal echocardiogram showing anechoic pericardial effusion surrounding the heart with visible right atrial collapse during diastole. (A) Echocardiography in parasternal long axis. Arrow shows the posterior displacement of the apex and the lack of the typical round left ventricular apex. Cardiovascular magnetic resonance showing the clockwise rotation. Compared with the prone position (B), leftward posterior rotation of the heart is seen in when patient is in supine position (C).
Reference:Pérez-Casares A, Cesar S, Brunet-Garcia L, Sanchez-de-Toledo J. Echocardiographic Evaluation of Pericardial Effusion and Cardiac Tamponade. Front Pediatr. 2017 Apr 24;5:79. doi: 10.3389/fped.2017.00079. PMID: 28484689; PMCID: PMC5401877.
Board Tip: Echocardiography has a sensitivity of 82% and specificity of 100% for detecting cardiac masses in dogs with pericardial effusion. However, masses may not be visible in cases of mesothelioma (diffuse disease) or early hemangiosarcoma. The pericardial effusion itself provides excellent acoustic contrast to help identify masses - so perform echo BEFORE pericardiocentesis if the patient is stable enough.
Pericardiocentesis: Emergency Treatment
Pericardiocentesis is the emergency treatment of choice for cardiac tamponade. When performed properly, it is associated with minimal complications and often provides dramatic clinical improvement.
Procedure Technique
- Patient positioning: Sternal or left lateral recumbency
- Site: Right hemithorax, 4th-6th intercostal space, just above costochondral junction
- Why right side?: Avoids left coronary artery; larger cardiac notch
- Equipment: 14-16 gauge over-the-needle catheter (fenestrated), extension set with 3-way stopcock, 60mL syringe
- Monitoring: Continuous ECG monitoring is essential
- Anesthesia: Local anesthesia (lidocaine) with or without light sedation
Fluid Analysis
Critical test: Does the fluid clot?
- Pericardial effusion: Will NOT clot (defibrinated blood)
- Cardiac chamber blood: WILL clot - indicates iatrogenic cardiac puncture
Submit samples for: PCV/TP, cytology, culture (if indicated), pH measurement.
High-Yield Note: Cytology has LOW diagnostic yield for cardiac tumors! Hemangiosarcoma and chemodectoma rarely exfoliate cells. Reactive mesothelial cells can mimic neoplasia (false positives). Do NOT rely on cytology alone to rule out neoplasia. Cytology is most useful for lymphoma and infectious causes.
Complications and Contraindications
- Potential complications: Cardiac puncture, arrhythmias (VPCs), coronary laceration, pneumothorax, tumor seeding
- Relative contraindication: Left atrial rupture (pericardiocentesis may promote continued bleeding) - consider supportive care first
Definitive Treatment and Prognosis
| Etiology | Treatment Options | Prognosis (MST) |
|---|---|---|
| Hemangiosarcoma | Pericardiocentesis (palliative) Pericardiectomy NOT recommended (hemorrhage risk) Chemotherapy (doxorubicin): modest benefit |
POOR Without treatment: 16 days Surgery + chemo: approximately 164 days High metastatic rate (greater than 90%) |
| Heart Base Tumor (Chemodectoma) | Subtotal pericardiectomy (recommended) Toceranib phosphate (Palladia) Radiation therapy (stereotactic) |
FAIR to GOOD With pericardiectomy: 730 days (2+ years) Without pericardiectomy: 42 days Slow growing, late to metastasize |
| Idiopathic Pericarditis | Pericardiocentesis (may be curative) Subtotal pericardiectomy after 3rd recurrence Corticosteroids not proven beneficial |
GOOD MST: 15-24 months Pericardiectomy is curative approximately 50% recur without surgery |
| Mesothelioma | Pericardiectomy (palliative) Chemotherapy (variable response) |
GUARDED MST: 6-14 months Often develops pleural effusion |
| PPDH | Surgical correction of hernia Many asymptomatic cases may not require surgery |
EXCELLENT Post-surgical prognosis excellent |
Board Tip: Key NAVLE distinction: Pericardiectomy is RECOMMENDED for heart base tumors and idiopathic pericarditis but NOT recommended for hemangiosarcoma (causes fatal intrathoracic hemorrhage). Remember: "Heart base = Help with surgery; Hemangiosarcoma = Hold off on pericardiectomy."
High-Yield Note: DIURETICS ARE CONTRAINDICATED in acute cardiac tamponade! Diuretics reduce preload, which is already critically low due to impaired ventricular filling. This will cause further decrease in cardiac output and worsen shock. The only effective treatment is pericardiocentesis to remove the mechanical compression.
Peritoneopericardial Diaphragmatic Hernia (PPDH)
PPDH is the most common congenital pericardial defect in dogs and cats. It results from incomplete development of the septum transversum, creating a communication between the pericardial and peritoneal cavities.
Key Features
- Breed predisposition: Weimaraners (may be inherited)
- Commonly herniated organs: Liver (most common), small intestine, omentum, spleen, stomach
- Associated defects: Umbilical hernia, sternal malformations, VSD
- Clinical signs: Often incidental finding; may have GI signs (vomiting, anorexia) or respiratory signs
- Diagnosis: Radiography (gas/soft tissue over heart), echocardiography, contrast studies
- Treatment: Surgical correction if symptomatic; asymptomatic cases may be monitored

Figure 6 - Lateral thoracic radiograph of a dog with PPDH showing gas-filled bowel loops overlying the cardiac silhouette and loss of the diaphragmatic line
Constrictive Pericarditis
Constrictive pericarditis is rare in dogs and typically develops as a sequela to chronic idiopathic pericarditis. The pericardium becomes thickened and fibrotic, restricting cardiac filling.
- Clinical signs: Similar to tamponade (ascites, jugular distension) but with NORMAL heart sounds and cardiac silhouette on radiographs
- Diagnosis: Difficult; may require cardiac catheterization; echo shows thickened pericardium
- Treatment: Surgical pericardiectomy (challenging as pericardium fused to epicardium)
- Prognosis: Guarded to poor
Summary: Key Takeaways
- Pericardial effusion is the most common pericardial disease in dogs (greater than 90% of cases)
- Leading causes: Neoplasia (hemangiosarcoma, chemodectoma) and idiopathic pericarditis
- Breed associations: Golden Retrievers/German Shepherds (hemangiosarcoma); Brachycephalics (chemodectoma)
- Cardiac tamponade causes right-sided heart failure signs (ascites, jugular distension)
- Classic findings: Beck's triad, pulsus paradoxus, globoid heart, electrical alternans
- Echocardiography is the gold standard diagnostic test
- Pericardiocentesis is the emergency treatment; performed from right hemithorax
- Diuretics are contraindicated in acute tamponade
- Pericardiectomy recommended for heart base tumors and idiopathic pericarditis, NOT for hemangiosarcoma
- PPDH is the most common congenital pericardial defect; Weimaraners predisposed
Practice Question
| A 9-year-old male neutered Golden Retriever presents with a 1-week history of lethargy, decreased appetite, and abdominal distension. On physical examination, you note muffled heart sounds, weak femoral pulses, distended jugular veins, and marked ascites. Thoracic radiographs reveal a globoid cardiac silhouette with sharp margins. Echocardiography confirms moderate pericardial effusion with right atrial collapse during diastole. A mass is visualized on the right auricular appendage. What is the most likely diagnosis, and what is the recommended initial treatment? A. Idiopathic pericarditis; subtotal pericardiectomy B. Right atrial hemangiosarcoma with cardiac tamponade; pericardiocentesis C. Chemodectoma with cardiac tamponade; furosemide and oxygen supplementation D. Dilated cardiomyopathy; pimobendan and furosemide E. Right atrial hemangiosarcoma with cardiac tamponade; immediate pericardiectomy |
|---|
Correct Answer: B
Explanation
Right atrial hemangiosarcoma with cardiac tamponade is the most likely diagnosis based on the signalment (older Golden Retriever), clinical presentation (signs of right-sided heart failure with muffled heart sounds and weak pulses indicating tamponade), and echocardiographic findings (pericardial effusion with a right auricular mass). The initial treatment should be pericardiocentesis to relieve the cardiac tamponade and restore cardiac output.
Option A (Idiopathic pericarditis; subtotal pericardiectomy) is incorrect because a mass was visualized on echocardiography, which rules out idiopathic pericarditis. Additionally, pericardiectomy would not be the initial treatment - emergency pericardiocentesis is required first.
Option C (Chemodectoma; furosemide and oxygen) is incorrect for two reasons: (1) Chemodectomas are heart BASE tumors, not right atrial masses, and are more common in brachycephalic breeds; (2) Furosemide is CONTRAINDICATED in cardiac tamponade as it further reduces preload and worsens hypotension.
Option D (Dilated cardiomyopathy) is incorrect because DCM would show a dilated, hypokinetic heart on echocardiography, not pericardial effusion with a mass. DCM also typically presents with a systolic murmur and often atrial fibrillation.
Option E (Immediate pericardiectomy) is incorrect because pericardiectomy is NOT recommended for hemangiosarcoma. It carries a high risk of fatal intrathoracic hemorrhage because there is no pericardium to contain bleeding from the tumor.
Board Tip: When you see an older Golden Retriever or German Shepherd with pericardial effusion and a right atrial mass, think HEMANGIOSARCOMA first. The initial treatment is always pericardiocentesis for cardiac tamponade. Remember that hemangiosarcoma has a poor prognosis with median survival of weeks to months even with treatment, and pericardiectomy is contraindicated due to hemorrhage risk. In contrast, if you see a Boxer or Boston Terrier with a heart BASE mass, think chemodectoma - these have a much better prognosis with pericardiectomy (MST greater than 2 years).
Image Sources
- Figure 1: Pericardial Anatomy Diagram - URL: https://microbenotes.com/pericardium-structure-functions/
- Figure 2: Pericardial Pressure-Volume Curve - PMC Open Access (CC BY 4.0). Source: "Pericardial Effusion: Overview of Aetiology, Pathophysiology, Diagnosis, and Management" URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC12515519/
- Figure 3: Thoracic Radiograph with Globoid Heart - PMC Open Access (CC BY 4.0). Source: "Acute severe pericarditis secondary to rodenticide intoxication in a dog" URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC9789774/
- Figure 4: ECG with Electrical Alternans - PMC Open Access (CC BY 4.0). Source: "Pericardial Effusion and Pericardiocentesis: Role of Echocardiography" URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC3518705/
- Figure 5: Echocardiogram with Pericardial Effusion - PMC Open Access (CC BY 4.0). Source: "Echocardiographic Evaluation of Pericardial Effusion and Cardiac Tamponade" URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC5401877/
- Figure 7: PPDH Radiograph - PMC Open Access (CC BY 4.0). Source: "Congenital peritoneopericardial diaphragmatic hernia in a terrier dog" URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC4279635/
References
- Shaw SP, Rush JE. Canine pericardial effusion: diagnosis, treatment, and prognosis. Compend Contin Educ Vet. 2007;29(7):405-411.
- Shaw SP, Rush JE. Canine pericardial effusion: pathophysiology and cause. Compend Contin Educ Vet. 2007;29(7):400-404.
- Merck Veterinary Manual. Pericardial Disease in Dogs and Cats. Available at: https://www.merckvetmanual.com/circulatory-system/various-heart-diseases-in-dogs-and-cats/pericardial-disease-in-dogs-and-cats
- Levi M, et al. Pathological Findings of Canine Idiopathic Pericarditis and Pericardial Mesotheliomas: Correlation with Clinical and Survival Data. Vet Sci. 2021;8(8):162.
- Ware WA, Hopper DL. Cardiac tumors in dogs: 1982-1995. J Vet Intern Med. 1999;13(2):95-103.
- Dunning D, et al. Analysis of prognostic indicators for dogs with pericardial effusion: 46 cases (1985-1996). J Am Vet Med Assoc. 1998;212(8):1276-1280.
- Aronsohn MG, et al. Cardiac tumors in the dog: A retrospective analysis and literature review. J Vet Intern Med. 2019;33(2):679-685.
- Stafford Johnson M, et al. Pericardial effusion in cats: a retrospective study of clinical findings and outcome in 146 cats. J Vet Intern Med. 2004;18(4):551-555.
- Morgan KRS, et al. Outcome after surgical and conservative treatments of canine peritoneopericardial diaphragmatic hernia: a multi-institutional study of 128 dogs. Vet Surg. 2020;49(1):138-145.
- dvm360. Pericardial disease: The forgotten cardiac malady. December 2024. Available at: https://www.dvm360.com/view/pericardial-disease-the-forgotten-cardiac-malady
Practice NAVLE Questions
Test your knowledge with 10,000+ exam-style questions, detailed explanations, and timed exams.
Start Your Free Trial →