Canine Cardiomyopathy Study Guide (1)
Canine Cardiomyopathy
NAVLE Study Guide
Cardiovascular System | Species: Canine
Estimated Read Time: 35-40 minutes | Last Updated: December 2024
Overview and Clinical Importance
Cardiomyopathies are primary diseases of the myocardium that result in structural and functional abnormalities of the heart muscle. In dogs, cardiomyopathies represent the second most common form of acquired heart disease after myxomatous mitral valve disease (MMVD) and are a leading cause of cardiac morbidity and mortality in large and giant breed dogs.
The three major types of canine cardiomyopathy include: Dilated Cardiomyopathy (DCM), the most common form; Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC), predominantly affecting Boxers; and Hypertrophic Cardiomyopathy (HCM), which is rare in dogs.
Learning Objectives
- Differentiate between dilated cardiomyopathy (DCM), arrhythmogenic right ventricular cardiomyopathy (ARVC), and hypertrophic cardiomyopathy (HCM)
- Identify breed predispositions for each type of cardiomyopathy
- Interpret echocardiographic and electrocardiographic findings in cardiomyopathy
- Develop appropriate treatment protocols for DCM and ARVC
- Understand the clinical significance of preclinical (occult) cardiomyopathy and screening recommendations
- Recognize diet-associated DCM and its relationship to grain-free diets
Dilated Cardiomyopathy (DCM)
Definition and Pathophysiology
Dilated cardiomyopathy is characterized by progressive ventricular chamber dilation and impaired systolic (contractile) function. The disease results from progressive loss of myocyte number and function, leading to decreased cardiac contractility. The left ventricle is most commonly affected, though biventricular involvement is frequently observed, particularly in giant breeds.
The pathophysiological sequence begins with myocardial dysfunction leading to decreased cardiac output. This triggers compensatory mechanisms including activation of the renin-angiotensin-aldosterone system (RAAS), sympathetic nervous system activation, and cardiac remodeling. Initially, these mechanisms maintain cardiac output, but over time they contribute to progressive chamber dilation, volume overload, and eventual congestive heart failure (CHF).
High-Yield Note: DCM has two distinct phases: the preclinical (occult) phase lasting 2-4 years with no clinical signs, and the clinical phase characterized by congestive heart failure with survival typically measured in weeks to months despite treatment.
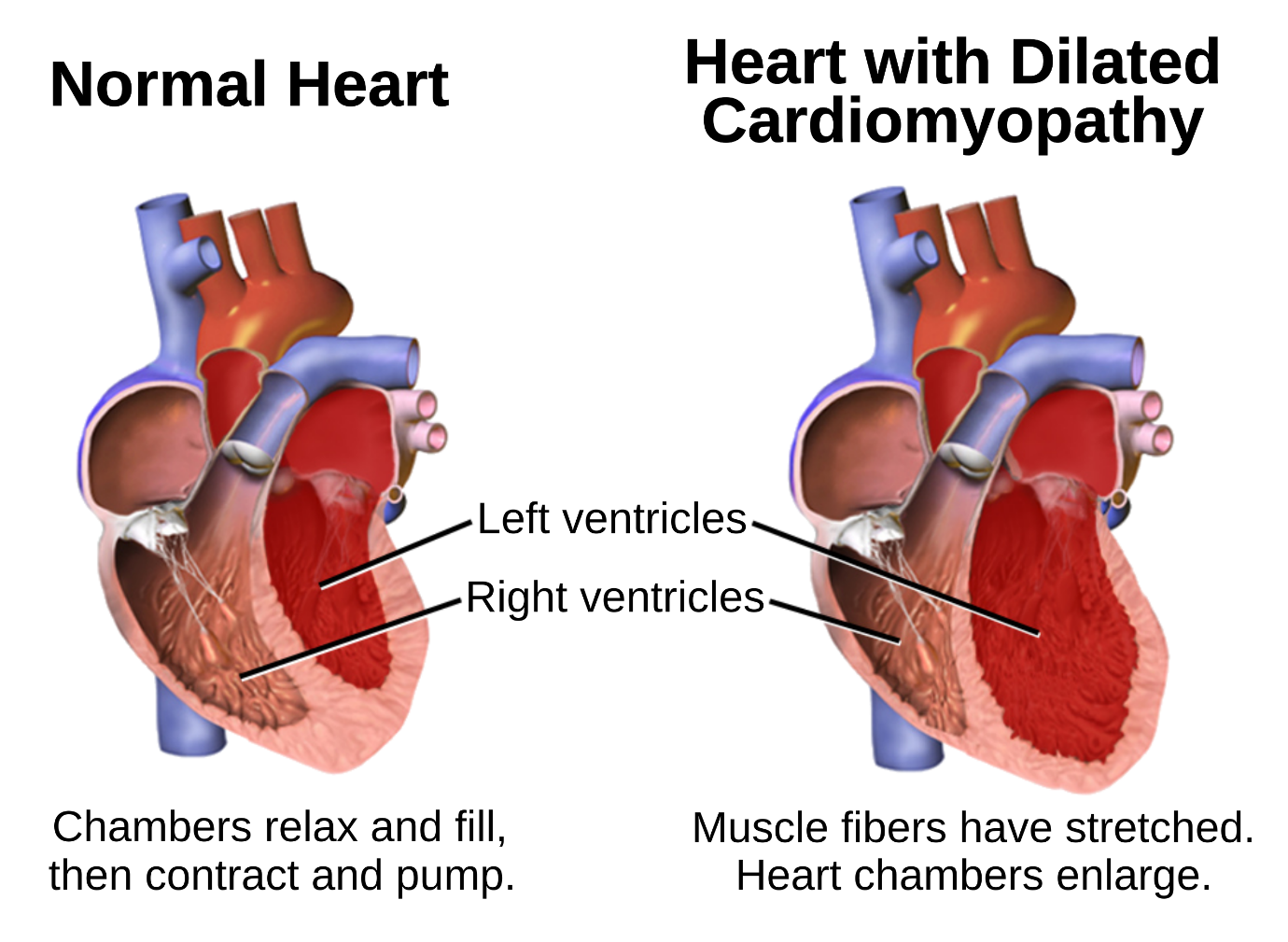
Figure 1 - Gross pathology image of a heart with dilated cardiomyopathy showing enlarged, globoid cardiac chambers with thinned ventricular walls compared to a normal heart
Breed Predispositions
DCM predominantly affects large and giant breed dogs, with certain breeds having well-documented genetic predispositions. The disease typically manifests in middle-aged to older dogs (4-10 years), with males often affected earlier and more severely than females.
| Breed | Prevalence/Characteristics | Special Considerations |
|---|---|---|
| Doberman Pinscher | 45-60% lifetime risk; males 50%, females 33% | High sudden death risk; ventricular arrhythmias common; PDK4 and TTN gene mutations |
| Irish Wolfhound | ~25% breed incidence; commonly develops atrial fibrillation | Pleural effusion common; 83% have concurrent atrial fibrillation |
| Great Dane | High prevalence; biventricular involvement common | Atrial fibrillation frequent; right-sided CHF with ascites |
| Cocker Spaniel | Taurine-responsive DCM; smaller breed exception | May improve with taurine supplementation; check taurine levels |
| Golden Retriever | Predisposed to taurine deficiency; diet-related DCM | Check whole blood taurine; diet history important |
| Boxer | Most develop ARVC rather than DCM; ~10% develop true DCM | L-Carnitine may be beneficial; STRN gene mutation |
Memory Aid: DCM Breed Predispositions
"DOGS WIIG" - Doberman, Other giants (Great Dane, Saint Bernard), Golden Retriever, Spaniel (Cocker), Wolfhound (Irish), Irish Setter, Intermediates (German Shepherd), German breeds (Schnauzer)
Clinical Presentation
Clinical signs of DCM depend on the stage of disease and whether congestive heart failure has developed. The preclinical phase may last years without obvious symptoms, making screening in high-risk breeds crucial.
Signs of Left-Sided Heart Failure
- Tachypnea and dyspnea (pulmonary edema)
- Coughing, particularly at night or with exercise
- Exercise intolerance and lethargy
- Orthopnea (difficulty breathing when lying down)
Signs of Right-Sided Heart Failure
- Ascites (abdominal distension)
- Jugular venous distension
- Pleural effusion (common in Irish Wolfhounds)
- Hepatomegaly and positive hepatojugular reflux
Physical Examination Findings
- Soft systolic murmur at left cardiac apex (mitral regurgitation from annular dilation)
- S3 gallop sound (best detected by experienced examiners)
- Weak, rapid femoral pulses with possible pulse deficits
- Arrhythmia (ventricular ectopy in Dobermans; atrial fibrillation in giant breeds)
Board Tip: A new heart murmur, gallop sound, or tachyarrhythmia detected in a large breed dog during routine examination should be considered a 'red flag' for occult DCM and warrants a complete cardiac workup including echocardiography.
Diagnosis
Echocardiography (Gold Standard)
Echocardiography is the definitive diagnostic test for DCM. Key findings include chamber dilation, decreased systolic function, and variable left atrial enlargement.
| Parameter | Normal Finding | DCM Finding |
|---|---|---|
| Fractional Shortening (FS%) | Greater than 25-30% | Less than 20% (often less than 15%) |
| LVIDd (diastole) | Breed/weight dependent | Increased (chamber dilation) |
| LVIDs (systole) | Breed/weight dependent | Markedly increased (impaired contraction) |
| EPSS | Less than 6-8 mm | Increased (poor contractility) |
| LA:Ao Ratio | Less than 1.6 | Greater than 1.6 (left atrial enlargement) |
Memory Aid - FS% Interpretation: 'FS under 20 means the heart can't do' - Fractional shortening less than 20% indicates significant systolic dysfunction consistent with DCM.
Electrocardiography and Holter Monitoring
ECG findings in DCM may include sinus tachycardia, atrial fibrillation (especially in giant breeds), ventricular premature complexes (VPCs), and left ventricular enlargement patterns (R wave greater than 3.5 mV in Lead II). Holter monitoring (24-hour ambulatory ECG) is particularly important in Dobermans where ventricular arrhythmias may precede echocardiographic changes by months to years.
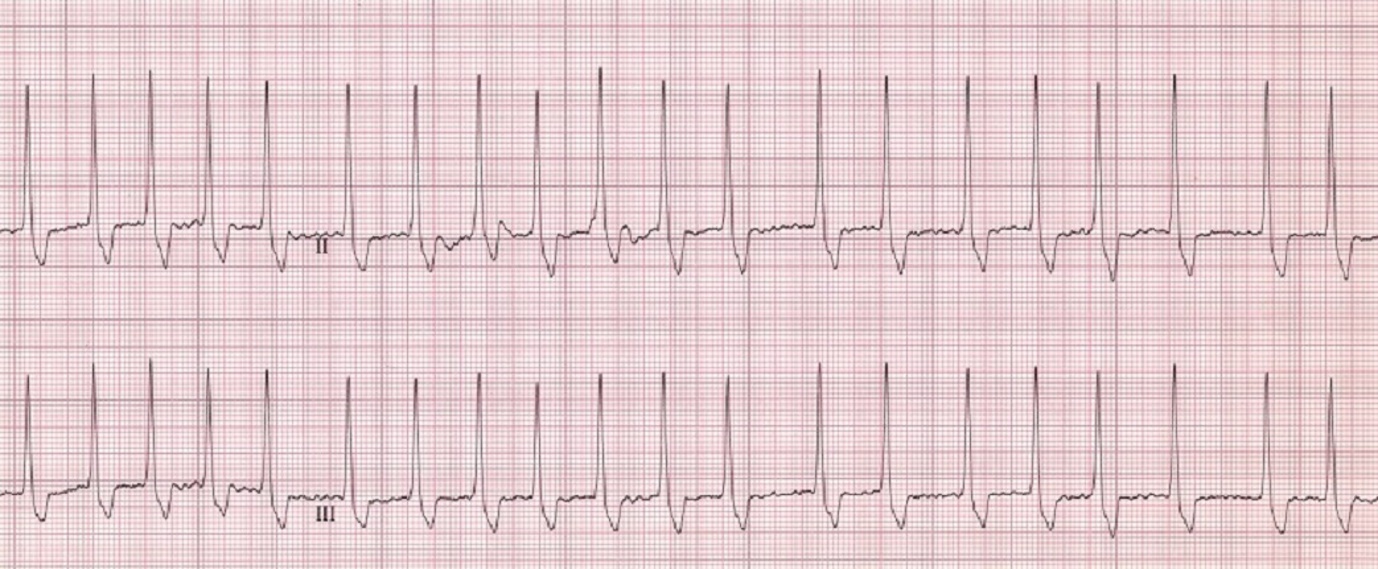
Figure 2 - ECG strip showing atrial fibrillation with irregular R-R intervals and absence of P waves in a dog with DCM]
Cardiac Biomarkers
- NT-proBNP: Elevated with volume overload and myocardial stretch; useful for screening and monitoring
- Cardiac Troponin I (cTnI): Indicates myocardial damage; may be elevated in active myocardial disease
- Taurine levels: Whole blood taurine should be measured in breeds susceptible to taurine-deficient DCM
Treatment of DCM
Preclinical (Occult) DCM
The landmark PROTECT study demonstrated that pimobendan treatment in Doberman Pinschers with preclinical DCM prolongs the time to onset of CHF or sudden death by approximately 9 months and extends overall survival.
High-Yield Note: The PROTECT study was the first to demonstrate that treating preclinical cardiac disease in dogs improves outcomes. Pimobendan is now indicated for preclinical DCM in Doberman Pinschers with echocardiographic evidence of disease.
Clinical DCM with Congestive Heart Failure
| Drug Class | Examples | Mechanism and Notes |
|---|---|---|
| Inodilator | Pimobendan 0.25-0.3 mg/kg PO q12h | Calcium sensitizer and PDE-III inhibitor; cornerstone of DCM therapy |
| Diuretics | Furosemide 2-4 mg/kg PO q8-12h | Essential for managing pulmonary edema and effusions |
| ACE Inhibitors | Enalapril 0.5 mg/kg PO q12h | Neurohormonal modulation; reduces afterload; monitor renal function |
| Antiarrhythmics | Sotalol, Mexiletine, Diltiazem | Selected based on arrhythmia type |
| Supplements | Taurine, L-Carnitine | For taurine/carnitine-responsive DCM; Cocker Spaniels, Golden Retrievers, Boxers |
Memory Aid: Doberman DCM
"Doberman = Double Doom" Double screening: Echo AND Holter annually starting at age 3-4 years Double trouble: VPCs greater than 300/24hr OR 50-300 on two consecutive Holters = concern Double-digit survival: Often only 3-6 months median survival after CHF develops
Prognosis
Prognosis for DCM varies significantly by breed and stage at presentation. Doberman Pinschers have the poorest prognosis, with median survival times of only 3-6 months after CHF develops. Other breeds may survive 6-24 months with appropriate treatment. Dogs with taurine-responsive DCM may have partial or complete reversal with supplementation and diet change.
Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)
Definition and Pathophysiology
Arrhythmogenic right ventricular cardiomyopathy (ARVC), formerly termed 'Boxer cardiomyopathy,' is a familial myocardial disease characterized by progressive replacement of normal myocardium with fibrous and adipose (fatty) tissue. This fibrofatty infiltration primarily affects the right ventricle and disrupts normal electrical conduction, leading to ventricular arrhythmias. Unlike DCM, the heart may appear structurally normal on echocardiography in approximately 90% of affected dogs.
ARVC is inherited as an autosomal dominant trait with incomplete penetrance. Two genetic mutations have been identified: STRN (Striatin) gene mutation (ARVC1) and a FOS gene mutation (ARVC2). Approximately 10% of affected Boxers will develop true DCM with systolic dysfunction.
High-Yield Note: ARVC primarily affects the electrical system of the heart, so the echocardiogram is often NORMAL. Diagnosis depends on Holter monitoring, not echocardiography. This is a key differentiation from DCM.
Clinical Presentation
The average age of onset for clinical symptoms is approximately 6 years, though the disease can manifest earlier or later. Clinical presentations fall into three categories:
- Asymptomatic with incidental arrhythmia: Detected during routine examination or screening
- Syncope (fainting): Occurs in approximately one-third of affected dogs, typically during exercise or excitement
- Sudden death: May occur without prior warning; results from VT degenerating into ventricular fibrillation
Diagnosis of ARVC
Holter Monitoring (24-Hour Ambulatory ECG)
Holter monitoring is the gold standard for ARVC diagnosis since the arrhythmia is often intermittent. Screening should begin at 3 years of age and be repeated annually.
| VPC Count (24 hours) | Interpretation |
|---|---|
| 0-50 VPCs (single, monomorphic) | Normal |
| 50-300 VPCs | Equivocal - repeat monitoring recommended |
| Greater than 100-300 VPCs with couplets, triplets, or VT | Diagnostic for ARVC |
| Greater than 1000 VPCs or ventricular tachycardia | Definitive ARVC; treatment indicated |
ECG Characteristics
The characteristic VPCs in ARVC are wide, upright (positive) complexes in leads I, II, III, and aVF, indicating a left bundle branch block (LBBB) morphology. This occurs because the abnormal impulse originates from the right ventricle.
Memory Aid - ARVC: "BOXER = B.O.X.E.R." Boxers (and Bulldogs) Origin: Right ventricle X-tra fat (fibro-fatty replacement) ECG shows VPCs with LBBB morphology (upright in lead II) Right ventricle origin = Left Bundle Branch Block pattern
Treatment of ARVC
Treatment decisions depend on the severity of arrhythmias and presence of symptoms. Not all ARVC cases require antiarrhythmic therapy.
Indications for Treatment
- Greater than 1000 VPCs per 24 hours
- Runs of ventricular tachycardia
- R-on-T phenomenon
- Clinical signs (syncope)
Antiarrhythmic Medications
| Drug | Dosage | Notes |
|---|---|---|
| Sotalol | 1.5-2.0 mg/kg PO q12h | First-line therapy; combined beta-blocker and Class III antiarrhythmic |
| Mexiletine | 5-6 mg/kg PO q8h WITH FOOD | Class IB antiarrhythmic; may cause GI upset - ALWAYS give with food |
| Atenolol | 12.5-25 mg/dog PO q12h | Beta-blocker; may be combined with mexiletine as alternative to sotalol |
Board Tip: When you see a Boxer with syncope, especially during exercise, and VPCs or VT with left bundle branch block morphology (upright in lead II), think ARVC first. The 24-hour Holter monitor is the gold standard for diagnosis, and sotalol is first-line treatment. Remember that echocardiography is often normal in ARVC.
Prognosis for ARVC
Prognosis for ARVC is highly variable. Many Boxers live for years on antiarrhythmic medication without symptoms, and some may even have normal lifespans. One study found median survival age of 11 years for ARVC dogs. However, sudden death remains a risk.
Diet-Associated Dilated Cardiomyopathy
Background and FDA Investigation
In July 2018, the FDA began investigating reports of DCM in dogs eating certain pet foods, particularly grain-free diets containing high proportions of peas, lentils, other legumes (pulses), and potatoes. These cases occurred in breeds not typically predisposed to DCM.
Key findings from the FDA investigation include:
- Greater than 90% of reported cases involved dogs eating grain-free diets
- 93% of implicated diets contained peas or lentils as main ingredients
- Golden Retrievers, Labrador Retrievers, and mixed breeds were commonly affected
- Not all affected dogs had taurine deficiency
High-Yield Note: Diet-associated DCM may be partially or fully reversible with diet change and taurine supplementation if caught early. Always obtain a complete diet history in any dog presenting with DCM, especially in breeds not typically predisposed.
Hypertrophic Cardiomyopathy (HCM)
Hypertrophic cardiomyopathy is extremely rare in dogs but occasionally seen in Boston Terriers and Bulldogs. HCM is characterized by thickening of the ventricular walls without chamber dilation, leading to impaired diastolic filling. Treatment focuses on beta-blockers or calcium channel blockers. This condition is far more common in cats.
Summary: Comparison of Canine Cardiomyopathies
| Feature | DCM | ARVC | HCM |
|---|---|---|---|
| Primary Breeds | Doberman, Great Dane, Irish Wolfhound | Boxer, English Bulldog | Boston Terrier (rare) |
| Echo Findings | Dilation, decreased FS% | Often NORMAL (90%) | Wall thickening |
| Key Diagnostic | Echocardiography | Holter monitoring | Echocardiography |
| First-Line Tx | Pimobendan, Furosemide | Sotalol | Beta-blocker |
Practice Question
| A 6-year-old male intact Boxer is presented for evaluation after experiencing two syncopal episodes during walks in the past week. The owner reports the dog briefly collapses, appears dazed for a few seconds, then recovers quickly. Physical examination reveals a heart rate of 140 bpm with an irregular rhythm. A 6-lead ECG reveals occasional wide, upright QRS complexes in lead II occurring singly and in short runs. An echocardiogram shows normal left ventricular dimensions and contractility with a fractional shortening of 35%. What is the most appropriate next diagnostic step? A. Cardiac catheterization B. 24-hour Holter monitoring C. Cardiac MRI D. Serum taurine levels E. NT-proBNP measurement |
|---|
Correct Answer: B
Explanation
24-hour Holter monitoring (B) is the most appropriate next step because this Boxer is presenting with clinical signs highly suggestive of arrhythmogenic right ventricular cardiomyopathy (ARVC). The combination of syncope during exercise, wide upright VPCs on ECG (indicating left bundle branch block morphology from right ventricular origin), AND a normal echocardiogram is classic for ARVC.
Option A (Cardiac catheterization) is incorrect because this invasive procedure is not indicated for the initial workup of suspected ARVC.
Option C (Cardiac MRI) is incorrect as the first diagnostic step. MRI requires general anesthesia and has limited availability.
Option D (Serum taurine levels) is incorrect because taurine deficiency is associated with DCM, not ARVC. This dog has a normal echocardiogram.
Option E (NT-proBNP measurement) is incorrect because this biomarker does not diagnose or characterize arrhythmias.
Clinical Pearl: In any Boxer presenting with syncope and VPCs, always think ARVC first. The normal echocardiogram is expected in ARVC since approximately 90% of affected dogs have normal cardiac structure. The diagnosis depends on Holter monitoring demonstrating greater than 100-300 VPCs/24 hours with couplets, triplets, or VT. If greater than 1000 VPCs or symptomatic, treatment with sotalol (first-line) should be initiated.
Key Takeaways
- DCM is the most common cardiomyopathy in dogs, affecting primarily large and giant breeds with ventricular dilation and systolic dysfunction diagnosed by echocardiography
- Doberman Pinschers have the highest prevalence of DCM and worst prognosis; annual screening with echo and Holter starting at age 3-4 is recommended
- ARVC primarily affects Boxers and is characterized by fibrofatty myocardial replacement causing ventricular arrhythmias; echocardiography is often NORMAL
- Holter monitoring is the gold standard for ARVC diagnosis; sotalol is first-line treatment for symptomatic arrhythmias
- Pimobendan is the cornerstone of DCM therapy and is indicated for both preclinical (Dobermans) and clinical DCM
- Diet-associated DCM may occur with grain-free diets containing legumes; obtain diet history and consider taurine levels in atypical cases
Image Sources
- Figure 1: https://en.wikipedia.org/wiki/Dilated_cardiomyopathy Figure 2: M-mode echocardiogram DCM - Animal Ultrasound Association Educational Resources. URL: https://www.animalultrasoundassociation.org/ (Educational use)
- Figure 2: https://www.merckvetmanual.com/multimedia/image/ecg-atrial-fibrillation-dog Figure 4: ARVC histopathology - PMC Open Access. Basso C, et al. Circulation. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC5953225/ (Creative Commons License)
References
- Summerfield NJ, et al. Efficacy of pimobendan in the prevention of congestive heart failure or sudden death in Doberman Pinschers with preclinical dilated cardiomyopathy (The PROTECT Study). J Vet Intern Med. 2012;26(6):1337-1349.
- Meurs KM, et al. Association of dilated cardiomyopathy with the striatin mutation genotype in boxer dogs. J Vet Intern Med. 2013;27(6):1437-1440.
- Wess G, et al. Prevalence of dilated cardiomyopathy in Doberman Pinschers in various age groups. J Vet Intern Med. 2010;24:533-538.
- Freeman LM, et al. Diet-associated dilated cardiomyopathy in dogs: what do we know? J Am Vet Med Assoc. 2018;253(11):1390-1394.
- Kaplan JL, et al. Taurine deficiency and dilated cardiomyopathy in golden retrievers fed commercial diets. PLoS One. 2018;13(12):e0209112.
- Merck Veterinary Manual. Dilated Cardiomyopathy in Dogs and Cats. 2024. URL: https://www.msdvetmanual.com/
- Cornell University College of Veterinary Medicine. Canine Dilated Cardiomyopathy. URL: https://www.vet.cornell.edu/
- FDA. Investigation into Potential Link between Certain Diets and Canine Dilated Cardiomyopathy. 2019. URL: https://www.fda.gov/
Practice NAVLE Questions
Test your knowledge with 10,000+ exam-style questions, detailed explanations, and timed exams.
Start Your Free Trial →