Canine Cardiac Arrhythmias
Canine Cardiac Arrhythmias
NAVLE Study Guide
Cardiovascular System | Species: Canine
Estimated Read Time: 35-40 minutes | Last Updated: December 2024
Overview and Clinical Importance
Cardiac arrhythmias are disturbances in the normal rhythm, rate, or electrical conduction of the heart. They represent a significant category of cardiovascular disease frequently tested on the NAVLE. Understanding arrhythmia classification, ECG interpretation, breed predispositions, and treatment protocols is essential for clinical practice and board examination success.
The heart's electrical activity normally originates from the sinoatrial (SA) node, which functions as the primary pacemaker. The impulse then travels through the atria, pauses at the atrioventricular (AV) node, and propagates through the bundle of His and Purkinje fibers to depolarize the ventricles. Disruption at any point in this pathway can result in an arrhythmia.
Learning Objectives
- Classify cardiac arrhythmias by origin (supraventricular vs. ventricular) and rate (tachycardia vs. bradycardia)
- Recognize ECG characteristics of common canine arrhythmias including atrial fibrillation, ventricular tachycardia, and AV block
- Identify breed predispositions for specific arrhythmias (Boxer ARVC, Doberman DCM, giant breed atrial fibrillation)
- Select appropriate antiarrhythmic medications based on arrhythmia type and hemodynamic status
- Determine when pacemaker implantation is indicated for bradyarrhythmias
Normal Canine ECG Parameters
Understanding normal ECG parameters is essential before identifying abnormalities. All measurements should be taken from Lead II at standard paper speed (50 mm/sec) and calibration (10 mm = 1 mV).
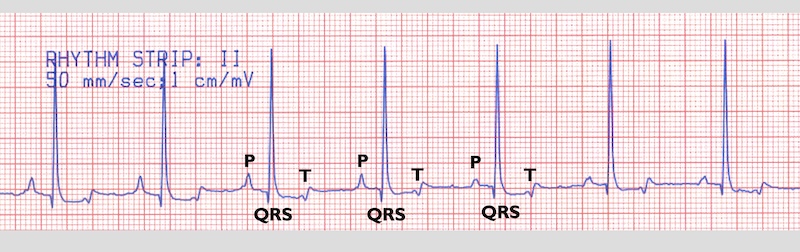
Figure 1 - Normal canine ECG
| Parameter | Normal Value | Clinical Significance |
|---|---|---|
| Heart Rate | 60-170 bpm | Smaller breeds have higher rates; toy breeds up to 180 bpm |
| P Wave Height | 0.4 mV or less | Greater than 0.4 mV suggests right atrial enlargement (P pulmonale) |
| P Wave Duration | 0.04-0.05 sec | Greater than 0.05 sec suggests left atrial enlargement (P mitrale) |
| PR Interval | 0.06-0.13 sec | Prolongation indicates first-degree AV block |
| QRS Duration | 0.05-0.06 sec | Greater than 0.06 sec suggests ventricular origin or bundle branch block |
| R Wave Amplitude | Up to 3.0 mV | Tall R waves may indicate left ventricular enlargement |
| T Wave | Variable polarity | May be positive, negative, or biphasic; all considered normal in dogs |
High-Yield Note: On the NAVLE, remember that ventricular arrhythmias produce wide, bizarre QRS complexes (greater than 0.06 sec) WITHOUT preceding P waves. Supraventricular arrhythmias have narrow, upright QRS complexes because they use the normal His-Purkinje conduction system.
Classification of Cardiac Arrhythmias
Arrhythmias are classified based on their site of origin and their effect on heart rate:
Arrhythmia Classification by Origin and Rate
| Category | Supraventricular Origin | Ventricular Origin |
|---|---|---|
| Tachyarrhythmias | Atrial fibrillation Supraventricular tachycardia Atrial flutter SVPCs (Supraventricular premature complexes) |
Ventricular tachycardia VPCs (Ventricular premature complexes) Ventricular fibrillation Accelerated idioventricular rhythm |
| Bradyarrhythmias | Sinus bradycardia Sick sinus syndrome Atrial standstill |
AV block (1st, 2nd, 3rd degree) Ventricular escape rhythm |
Tachyarrhythmias
Atrial Fibrillation (AF)
Atrial fibrillation is the most common sustained arrhythmia in dogs. It is characterized by rapid, chaotic electrical activation of the atria (greater than 600 depolarizations per minute) without organized atrial contraction. The AV node filters these impulses, allowing only some to conduct to the ventricles, resulting in an irregularly irregular ventricular rhythm.
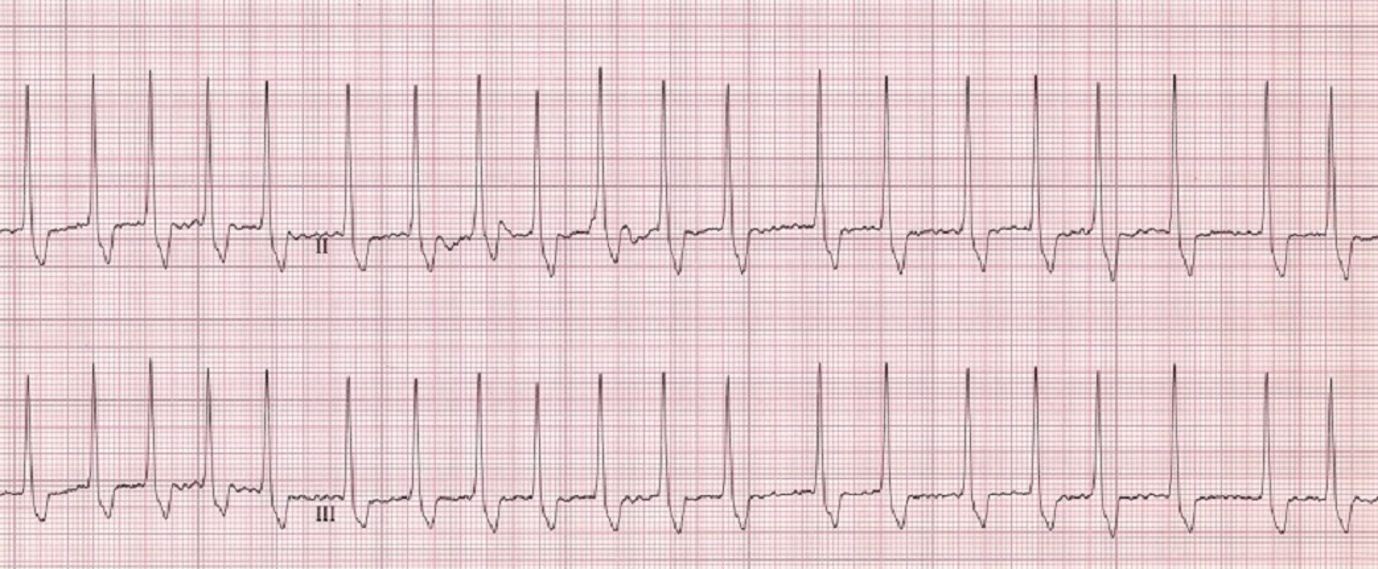
Figure 2 - This ECG of a dog shows a fast ventricular rate (230 bpm) and an irregular rhythm. The complexes are supraventricular (normal). There are no P waves. This combination is diagnostic of atrial fibrillation.
Courtesy of Dr. Mark D. Kittleson
ECG Characteristics
- Absence of P waves - replaced by irregular baseline undulations (fibrillation waves or f waves)
- Irregularly irregular R-R intervals - no pattern to the irregularity
- Narrow QRS complexes - normal morphology because conduction uses His-Purkinje system
- Rapid ventricular rate - often greater than 200-220 bpm without treatment
Clinical Presentation and Breed Predispositions
AF most commonly occurs secondary to severe atrial enlargement from underlying structural heart disease (dilated cardiomyopathy, degenerative mitral valve disease). However, "Lone AF" can occur in large and giant breed dogs without structural heart disease due to their naturally large atrial mass and high vagal tone.
Predisposed breeds: Great Danes, Irish Wolfhounds, Newfoundlands, Doberman Pinschers, Boxers (with DCM), and other giant breeds weighing greater than 40 kg.
Treatment
The goal of treatment is rate control (target: average heart rate less than 125-160 bpm) rather than rhythm control, as cardioversion is rarely successful in dogs with underlying heart disease.
- Diltiazem + Digoxin combination: Most effective for rate control. Diltiazem (calcium channel blocker) 1.5-2.5 mg/kg PO q8h + Digoxin 0.003-0.005 mg/kg PO q12h
- Beta-blockers: Atenolol or sotalol may be used for lone AF in giant breeds
- Also treat underlying heart disease and congestive heart failure if present
Board Tip: When you see an ECG with an irregularly irregular rhythm, absent P waves, and narrow QRS complexes - think AF immediately. On auscultation, AF sounds "chaotic" or like "tennis shoes in a dryer." Remember that adequate rate control (HR less than 160 bpm) significantly improves survival compared to inadequate control.
Ventricular Premature Complexes (VPCs) and Ventricular Tachycardia
Ventricular premature complexes (VPCs) originate below the AV node within the ventricular myocardium. Because they bypass the normal His-Purkinje conduction system, VPCs produce wide, bizarre QRS complexes. When three or more consecutive VPCs occur at a rate greater than 100 bpm, this is termed ventricular tachycardia (VT).
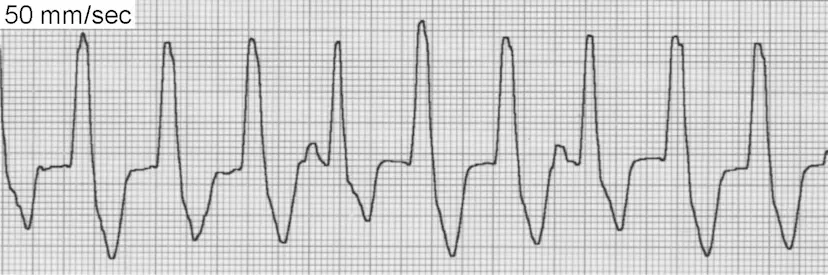
Figure 3 - ECG showing ventricular tachycardia with wide, bizarre QRS complexes
ECG Characteristics of VPCs/VT
- Wide QRS complexes (greater than 0.06 sec) with bizarre morphology
- No preceding P wave associated with the VPC
- T wave opposite in direction to the main QRS deflection
- Compensatory pause typically follows the VPC
- VPC morphology indicates origin: Upright (positive) VPCs in lead II suggest right ventricular origin; negative VPCs suggest left ventricular origin
Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)
ARVC (also known as Boxer Cardiomyopathy) is a genetic disease characterized by progressive fibro-fatty replacement of the right ventricular myocardium. This creates substrate for ventricular arrhythmias. ARVC is inherited in an autosomal dominant pattern with variable penetrance.
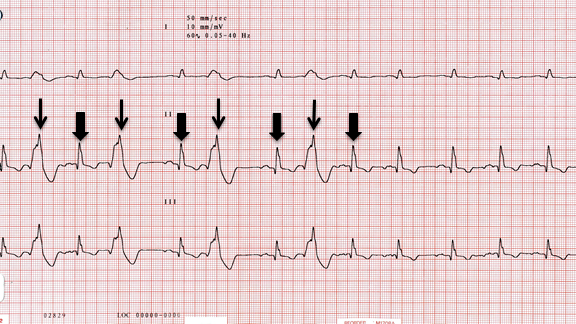
Figure 4 - ECG from Boxer with ARVC
Clinical Features
- Breed predisposition: Boxers (classic), English Bulldogs, German Shepherds
- Clinical signs: Syncope (especially during exercise or excitement), weakness, sudden death
- ECG findings: VPCs with LEFT bundle branch block (LBBB) morphology - upright (positive) in leads II, III, aVF because they originate from the right ventricle
- Echocardiography: Often NORMAL because the disease is primarily electrical; some dogs develop RV dilation or DCM phenotype
- Holter diagnostic criteria: Greater than 100-300 VPCs in 24 hours is diagnostic in Boxers
Treatment of ARVC
- First-line: Sotalol 1-3 mg/kg PO q12h (beta-blocker with class III antiarrhythmic properties)
- Alternative: Mexiletine + Atenolol combination - Mexiletine 5-10 mg/kg PO q8h WITH FOOD + Atenolol 12.5-25 mg/dog PO q12h
- Fish oil supplementation may reduce arrhythmia frequency
- Goal: Greater than 85% reduction in VPC frequency on repeat Holter
Memory Aid - ARVC: "BOXER = B.O.X.E.R."
Boxers (and Bulldogs) are predisposed
Origin: Right ventricle
X-tra fat (fibro-fatty replacement of myocardium)
ECG shows VPCs with LBBB pattern (upright in lead II)
Right ventricle origin means LBBB morphology!
Board Tip: When you see a Boxer with syncope, especially during exercise, and VPCs or VT with left bundle branch block morphology (upright in lead II), think ARVC first. The 24-hour Holter monitor is the gold standard for diagnosis, and sotalol is first-line treatment. Remember that echocardiography is often normal in ARVC because the disease causes primarily electrical rather than structural abnormalities in early stages.
Dilated Cardiomyopathy with Arrhythmias (Doberman Pinscher)
Doberman Pinschers have a unique form of dilated cardiomyopathy (DCM) with both systolic dysfunction AND an arrhythmogenic component. Up to 45% of Dobermans in the U.S. may be affected. The disease has a prolonged occult (preclinical) phase before clinical signs of heart failure appear.
Screening Recommendations (European Society of Veterinary Cardiology)
- Begin screening at 3 years of age
- Annual screening with BOTH echocardiography AND 24-hour Holter monitor
- Holter criteria for occult DCM: Greater than 300 VPCs/24h is diagnostic; 50-300 VPCs on two consecutive recordings is also diagnostic
- Less than 50 VPCs/24h is considered normal, but ANY VPCs warrant monitoring
Memory Aid - "Doberman = Double Doom"
Double screening: Echo AND Holter annually starting at age 3
Double trouble: VPCs greater than 300/24hr OR 50-300 on two consecutive readings = diagnostic
Double-digit survival: Only 3-6 months median survival after CHF develops
Bradyarrhythmias
Sick Sinus Syndrome (SSS)
Sick sinus syndrome is a constellation of abnormalities involving the sinoatrial node, including inappropriate sinus bradycardia, sinus arrest, and alternating bradycardia-tachycardia episodes. It is the second most common indication for pacemaker implantation in dogs.

Figure 5 - This ECG of a dog shows sinus arrest followed by a ventricular escape beat (VEB), an atrial premature complex (APC), and second-degree AV block.
Courtesy of Dr. Mark D. Kittleson.
Breed Predispositions
Miniature Schnauzers (especially females), West Highland White Terriers, Cocker Spaniels, Dachshunds, and Pugs. Typically affects middle-aged to older dogs.
ECG Features
- Sinus bradycardia - heart rate less than 40-60 bpm
- Sinus arrest - pause greater than 2x normal R-R interval; if greater than 8 seconds, syncope occurs
- Escape beats - junctional or ventricular complexes that "rescue" the heart during long pauses
- Bradycardia-tachycardia syndrome - alternating slow and fast rhythms (often supraventricular tachycardia)
Clinical Signs
The most common presenting sign is syncope (95% of symptomatic cases). Other signs include episodic weakness, lethargy, and exercise intolerance. Some dogs are asymptomatic and diagnosed incidentally.
Diagnosis and Treatment
- Atropine response test: 0.04 mg/kg IV - a positive response (increased HR) suggests vagally-mediated component and predicts response to medical therapy
- Medical therapy: Propantheline, theophylline, or terbutaline may help dogs with positive atropine response
- Pacemaker implantation: Treatment of choice for symptomatic SSS; 90% of dogs have complete resolution of syncope post-pacemaker
High-Yield Note: Never suppress escape beats in a dog with SSS - they are keeping the dog alive! Dogs with SSS are high-risk anesthetic candidates due to potential for prolonged sinus arrest. If anesthesia is necessary, temporary pacing should be considered.
Atrioventricular Block
AV block occurs when electrical impulses from the atria are delayed or blocked at the AV node. There are three degrees of severity:
| Degree | ECG Finding | Clinical Significance | Treatment |
|---|---|---|---|
| 1st Degree | Prolonged PR interval (greater than 0.13 sec); all P waves conduct | Usually benign; often due to high vagal tone or drugs | None required if asymptomatic |
| 2nd Degree | Some P waves not followed by QRS (intermittent conduction failure) | Mobitz I (Wenckebach): progressive PR prolongation - usually benign Mobitz II: constant PR with dropped beats - more serious |
High-grade Mobitz II may require pacemaker |
| 3rd Degree (Complete) | Complete AV dissociation; P waves and QRS complexes occur independently | Ventricular escape rhythm (20-40 bpm); high risk of syncope and sudden death | PACEMAKER - only effective treatment |
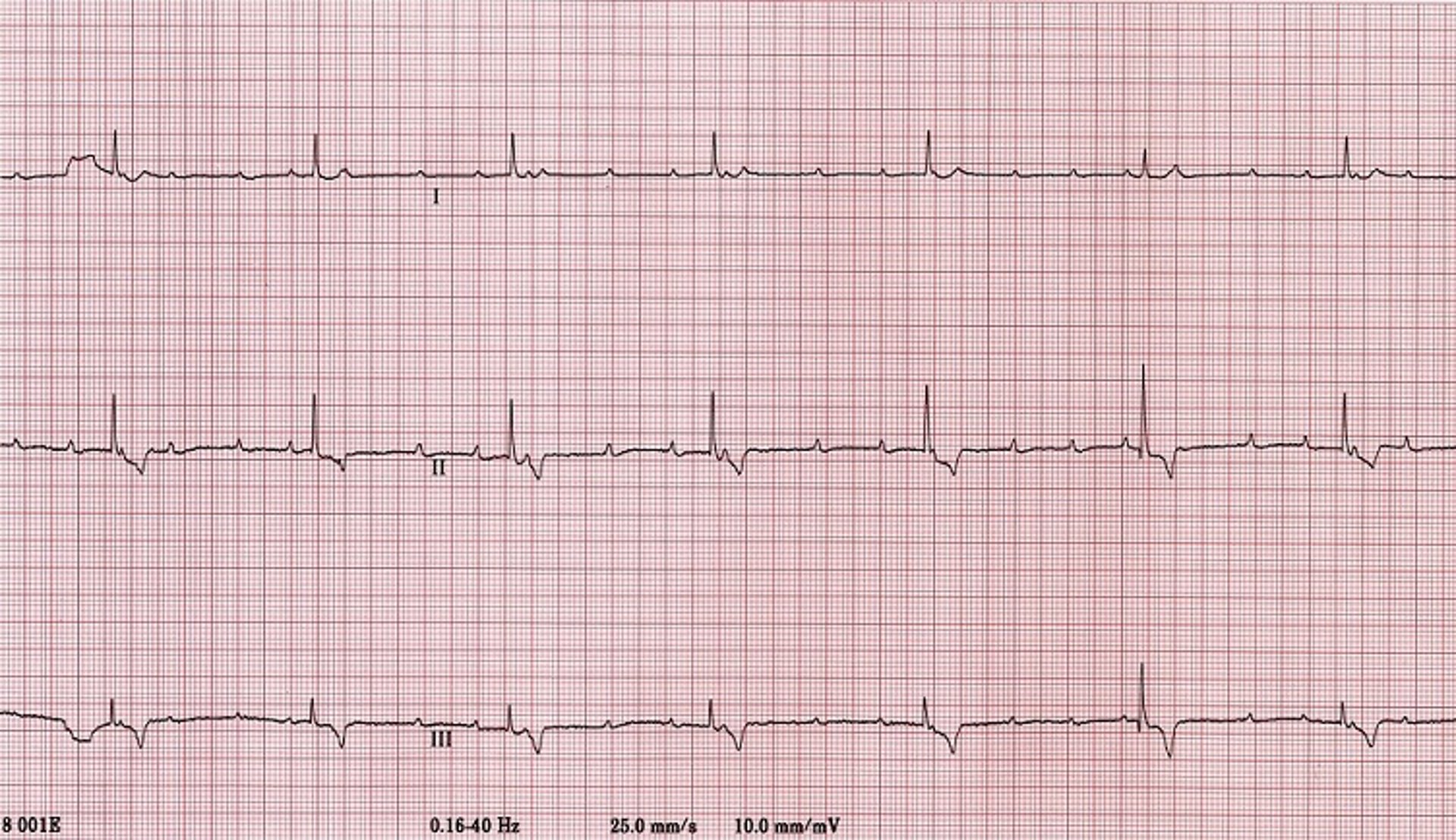
Figure 6 - In this ECG of a dog, the P waves and QRS complexes (R) are dissociated from one another (there is no apparent relationship between them). The atrial rate varies from ~100 to 150 bpm (P-P interval varies from 0.6 to 0.4 second), and the ventricular rate is steady and in the low 40s (R-R interval = 1.46 seconds), with normal QRS-T complexes (nodal escape rhythm).
Courtesy of Dr. Mark D. Kittleson.
Board Tip: Third-degree AV block is the most common indication for pacemaker implantation in dogs. Key ECG finding: P waves "march through" at their own rate while QRS complexes occur at a slower, independent rate. Dogs are at risk for sudden death even if asymptomatic. Breeds predisposed include Cocker Spaniels, Pugs, Labrador Retrievers, and Chow Chows.
Antiarrhythmic Drug Summary
| Drug | Class | Primary Use | Dosage | Key Points |
|---|---|---|---|---|
| Lidocaine | Class IB (Na+ channel blocker) | Acute VT (IV only) | 2-4 mg/kg IV bolus; CRI 30-90 mcg/kg/min | First-line for emergency VT; max cumulative dose 6-8 mg/kg |
| Mexiletine | Class IB | Chronic ventricular arrhythmias | 5-10 mg/kg PO q8h WITH FOOD | Oral lidocaine analog; give with food to reduce GI upset |
| Sotalol | Class III + Beta-blocker | VT, ARVC | 1-3 mg/kg PO q12h | First-line for ARVC; avoid in CHF (negative inotropy) |
| Diltiazem | Class IV (Ca2+ channel blocker) | AF rate control, SVT | 1.5-2.5 mg/kg PO q8h | Slows AV conduction; combine with digoxin for AF |
| Digoxin | Cardiac glycoside | AF rate control | 0.003-0.005 mg/kg PO q12h | Narrow therapeutic index; monitor serum levels (0.5-0.9 ng/mL) |
| Atenolol | Class II (Beta-blocker) | Rate control, lone AF | 0.5-2 mg/kg PO q12-24h | Often combined with mexiletine for ARVC |
Breed Predispositions Summary
| Breed | Arrhythmia | Key Feature |
|---|---|---|
| Boxer | ARVC with VT | VPCs with LBBB morphology; normal echo |
| Doberman Pinscher | DCM with VPCs, AF | Annual Echo + Holter screening from age 3 |
| Great Dane, Irish Wolfhound | Atrial Fibrillation | Can have "Lone AF" without structural disease |
| Miniature Schnauzer | Sick Sinus Syndrome | Females predisposed; pacemaker often needed |
| Cocker Spaniel | SSS, 3rd degree AV block | Both bradyarrhythmias common |
| German Shepherd | Inherited ventricular arrhythmia | Affects young dogs; resolves by 24 months |
Practice Question
| A 7-year-old male neutered Boxer presents with a 3-week history of exercise intolerance and two syncopal episodes during walks. The owner reports that during both episodes, the dog collapsed suddenly, was unresponsive for approximately 10 seconds, and then recovered quickly. On physical examination, the dog is bright and alert with pink mucous membranes. Auscultation reveals an irregular rhythm with occasional pauses. An ECG reveals wide, bizarre QRS complexes occurring in runs of 5-8 beats at a rate of 240 bpm, alternating with periods of normal sinus rhythm. The VPCs are upright (positive) in leads II, III, and aVF. Echocardiography shows normal chamber dimensions and systolic function. What is the most likely diagnosis? A. Atrial fibrillation secondary to dilated cardiomyopathy B. Sick sinus syndrome with bradycardia-tachycardia C. Arrhythmogenic right ventricular cardiomyopathy (ARVC) D. Third-degree atrioventricular block E. Supraventricular tachycardia |
|---|
Correct Answer: C
Explanation
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is the correct diagnosis based on several classic features present in this case:
- Breed: Boxers are the classic breed affected by ARVC
- Clinical presentation: Exercise-induced syncope is characteristic of ARVC due to ventricular tachycardia compromising cardiac output
- ECG findings: Wide, bizarre QRS complexes (ventricular origin) that are upright in leads II, III, and aVF indicate LEFT bundle branch block (LBBB) morphology, meaning the arrhythmia originates from the RIGHT ventricle
- Normal echocardiogram: This is KEY - ARVC often presents with normal chamber dimensions and systolic function because it is primarily an electrical disease early in its course
Why the other options are incorrect:
Option A (Atrial fibrillation secondary to DCM) is incorrect because AF presents with narrow QRS complexes (supraventricular), absent P waves, and an irregularly irregular rhythm. Additionally, the echocardiogram would show chamber enlargement with DCM.
Option B (Sick sinus syndrome) is incorrect because SSS primarily causes bradycardia with sinus arrest and escape beats. While bradycardia-tachycardia can occur, the tachycardia is typically supraventricular (narrow QRS), not ventricular (wide QRS). SSS also predominantly affects Miniature Schnauzers and other small breeds.
Option D (Third-degree AV block) is incorrect because third-degree AV block causes profound bradycardia (20-40 bpm) with a slow ventricular escape rhythm, not tachycardia. The ECG would show P waves marching independently of slow, wide QRS complexes.
Option E (Supraventricular tachycardia) is incorrect because SVT produces narrow, upright QRS complexes since the impulse uses the normal His-Purkinje conduction system. The wide, bizarre QRS complexes in this case indicate ventricular origin.
Clinical Pearl: In any Boxer presenting with syncope or exercise intolerance, ARVC with ventricular arrhythmias should be high on your differential list. A 24-hour Holter monitor is the gold standard for diagnosis (greater than 100-300 VPCs/24h is diagnostic). Remember: a normal echocardiogram does NOT rule out ARVC! Treatment with sotalol (1-3 mg/kg PO BID) is first-line and effectively reduces VPC frequency and syncope in most cases.
Summary: Key Takeaways
- Classify arrhythmias by origin: Supraventricular arrhythmias have narrow QRS complexes; ventricular arrhythmias have wide, bizarre QRS complexes
- Atrial fibrillation: Irregularly irregular rhythm, absent P waves, narrow QRS; treat with diltiazem + digoxin for rate control
- ARVC in Boxers: VPCs with LBBB morphology (upright in lead II), normal echo, syncope; treat with sotalol
- Doberman DCM: Screen with both Echo AND Holter starting at age 3; greater than 300 VPCs/24h or 50-300 on two consecutive Holters is diagnostic
- Sick sinus syndrome: Miniature Schnauzers, syncope due to sinus arrest; pacemaker is definitive treatment
- Third-degree AV block: Complete AV dissociation, bradycardia 20-40 bpm; PACEMAKER is the only effective treatment
- Lidocaine: First-line IV drug for acute ventricular tachycardia
- Never suppress escape beats: They are keeping the patient alive during bradyarrhythmias!
Image Sources
The following free-use and open-access sources are recommended for obtaining images:
- Figure 1 - Normal Canine ECG: MSD Veterinary Manual - Canine ECG Interpretation. URL: https://www.msdvetmanual.com/circulatory-system/cardiovascular-system-introduction/the-cardiovascular-system-in-animals)
- Figure 2 - Atrial Fibrillation ECG: MSD Veterinary Manual - ECG, Atrial Fibrillation, Dog. URL https://www.msdvetmanual.com/multimedia/image/ecg-atrial-fibrillation-dog (Open access educational resource)
- Figure 3 - Ventricular Tachycardia ECG: Clinician's Brief - Interpreting ECGs with Confidence. URL: https://www.cliniciansbrief.com/article/interpreting-ecgs-confidence-part-1 (Open access veterinary education)
- Figure 4 - ARVC in dogs: https://www.uvsonline.com/arvc-in-dogs/
- Figure 5 - Sick Sinus Syndrome ECG: Heart Disease: Conduction Abnormalities in Dogs and Cats accessed from https://www.merckvetmanual.com/
- Figure 6 - Third-Degree AV Block ECG: MSD Veterinary Manual - Heart Disease: Conduction Abnormalities. URL: https://www.msdvetmanual.com/circulatory-system/heart-disease-conduction-abnormalities-in-dogs-and-cats/ (Open access educational resource)
References
- Gelzer AR, Kraus MS, Rishniw M, et al. Combination therapy with digoxin and diltiazem controls ventricular rate in chronic atrial fibrillation in dogs better than digoxin or diltiazem monotherapy. J Vet Intern Med. 2009;23:499-508.
- Wess G. Screening for dilated cardiomyopathy in dogs. J Vet Cardiol. 2022;40:51-68.
- Meurs KM. Arrhythmogenic right ventricular cardiomyopathy in the Boxer dog. Vet Clin North Am Small Anim Pract. 2017;47(5):1103-1111.
- Ward J, Schober KE, Fuentes VL. Outcome and survival in dogs with sick sinus syndrome and sinus node dysfunction: 93 cases (2002-2014). J Vet Intern Med. 2016;30:1505-1513.
- Tilley LP, Smith FWK. Essentials of Canine and Feline Electrocardiography: Interpretation and Treatment. 3rd ed. Philadelphia: Lea & Febiger; 1992.
- Scansen BA, Meurs KM, Spier AW, et al. Temporal variability of ventricular arrhythmias in Boxer dogs with arrhythmogenic right ventricular cardiomyopathy. J Vet Intern Med. 2009;23:1020-1024.
- Wess G, Domenech O, Dukes-McEwan J, et al. European Society of Veterinary Cardiology screening guidelines for dilated cardiomyopathy in Doberman Pinschers. J Vet Cardiol. 2017;19:405-415.
- MSD Veterinary Manual. Heart Disease: Conduction Abnormalities in Dogs and Cats. Available at: https://www.msdvetmanual.com/circulatory-system/heart-disease-conduction-abnormalities-in-dogs-and-cats/
- Cornell University College of Veterinary Medicine. Arrhythmias (Abnormal Rhythms) in Dogs. Available at: https://www.vet.cornell.edu/hospitals/services/cardiology/arrhythmias-abnormal-rhythms-dogs
- Sleeper MM. Reading ECGs in veterinary patients: an introduction. dvm360. 2024. Available at: https://www.dvm360.com/view/reading-ecgs-in-veterinary-patients-an-introduction
Practice NAVLE Questions
Test your knowledge with 10,000+ exam-style questions, detailed explanations, and timed exams.
Start Your Free Trial →